Sexually Transmitted Diseases- Ten Years Experience In Benue State
E Okwori, O Alao
Citation
E Okwori, O Alao. Sexually Transmitted Diseases- Ten Years Experience In Benue State. The Internet Journal of Third World Medicine. 2008 Volume 8 Number 1.
Abstract
Introduction
Inflection by a number of viruses, bacteria, fungi, protozoa or anthropods are transmitted through heterosexual or homosexual contact. These sexually transmitted infection ( STD) can result in a wide variety of Clinical conditions. STDs rank among the most frequent infectious disease ( 1,2) . The world Health organization in(1995) estimated the incidence of four selected curable sexually transmitted disease – gonorrhea, syphilis, Chlamydia and triclononiasis among adults age 15 – 49 at 333million of these , the vast,. majority (3) occurred in the developing world (3). 45% in south and South East Asia, 20% in sub-Saharan Africa and 11% in Latin America and the Caribbean countries (3).
Epidemiological data in the developing countries is not easy available.
STD are also the most international of all diseases affecting mankind and in the all countries they are of major social and public health importance ( 3,4,5). In Nigeria some workers, mostly from the Southern part of thee country did much work on these diseases 96,7) in the north central Nigeria information on STD is very scanty. This work will form a data base in the area. Benue State is located in the central of Nigeria. It has eighteen local government areas. Makurdi is the capital of the state with two other urban areas. Otukpo and Gboko. In Benue state beside malaria and gastrointestinal disease, STDs are the complaints for which adolescents and adults seek medical attention.
The present report is based on Clinical and laboratory findings on patients attending federal Medical Centre Makurdi, General hospital Otukpo, and a private Clinic at Makurdi from January 1999-Dec. 2008.
Human immune deficiency Virus (HIV) prevalence in the area is high almost ten thousand (10,000) are attending HIV Clinics in the State, which is separate from STD Clinic. That work had already been published by the same author.
Materials And Method
All the patients who attended the STD Clinics of FMC – Mkd, general hospital Otukpo and a private clinic in Makurdi between January 1999 and Dec. 2008 were included in this study.
All the patients gave their full consent after proper counseling. And they were subjected to full physical examination after relevant histories had been taken.
Samples of urethral discharge in men and endocervial swab in women were taken using sterile cotton swabs. The smears were gram-strained and a culture plate inoculated. On
plates of chocolate and Thayer Martin (Oxoid) media. The plates were incubated at 37oc in a candle extinction jar for 24 to 48 hours. Neisseria gonorrhea was identified by the typical colonial appearance, reactions to gram stain, positive Oxidase test and sugar ternentatanin.
The antibiotic sensitivity of isolates was tested by the agar diffusion method on chocolates agar plates using Oxoid multidiscs with standard antibiotics concentration. Penicillinase production was detected by starch paper method of Odugbemi method (14). Candida was diagnosed by culture on chocolate agar and sahouraud agar or both and by microcospy of a saline-mount and gram-stained smear of material from vagina. Dank field microcopy was performed on genital ulcers. Diagnosis of Trichomonas was by direct microcopy. Lyphogranuloma venerum (LGV), genital herpes, chancroid and Molluscum contagiosum were diagnosed clinically. The veneral disease research laboratory (VDRL), and Trepanoma pallidum Haematiglutination (TPHA) were used to diagnose syphilis.
Results
One thousand four hundred and forty eight (1,448) or 61.07%) males and nine hundred and twenty three (923or 38.93) females were seen in the Clinics at General out patients and Sexually Transmitted Diseases Clinics (STD). Treatment clinics (STI) during the ten years period at Otukpo general hospital, federal medical centre, Makurdi and Marian Clinic Makurdi.
This represents a male to female ratio of 2:1.
The peak age for men a was 31 – 40 years while that women was 21-30 years (tableI)
The non gonococcus infection and gonorrhea and chancroid were the three most common STDs seen in Benue State, each accounting for 38.86%, 9.50% and 9.07% respectively (tableII). Casual Sexual contact and commercial sex work (CSWs) were the sources of infection in 50.09% and 35.15%) respectively of the clients (table III).
Distribution of the STD by occupation showed that civil servants, drivers, and tertiary Schools Students accounted for 28.41%, 26.94% and 22.63% respectively. (Table IV).
Ninety seven percent (97%) of the neisseria gonorrhea isolated were penicillinase producing neisseria gonorrhea.
Figure 1

Figure 2
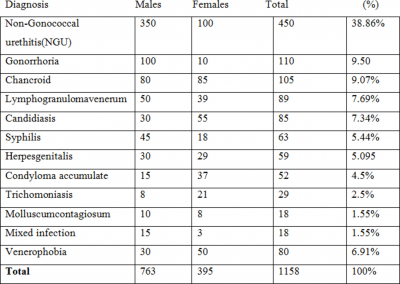
Figure 3

Figure 4

Discussion
One thousand nine hundred and thirty two (1932 or 81.485) of the patients in this study were aged 11 and 40years. This study were agrees with the Jos figure (92%) but in disagreement with Zaria, Ibadan and Lagos figure (61%, 51%, and 40% respectively.
This difference was probably because most of our patients were civil servants and Students. The age group 11- 40 years is the sexually active age group, thus are more at risk of acquiring STDs .
They are also assumed to have higher level of awareness.
Sixty three (63 or 9.07%) of the clients were serologically reactive for syphilis. Ilorin reported 12% of syphilis cases, but Sogbetum reported 2.5% syphilis cases in Ibadan.
Gonorrhea was more frequent among males (8.64%) than in female (0.86%) attending the Clinics. This agrees with the reports from Jos, Zaria, and Ilorin (14, 15). The low incidence among female is because female are often symptomless and act as carriers.
Eighty (80-or 6.91%) of the patients presented with venerophobia. We observed that these group of patients engage in self medications and had history of been seen by many Doctors and non doctors before presenting to us.
Self medications and indiscriminate use of antibiotic increase the resistance of the bacteria to antibiotics. Illustrations of the negative effect of socio cultural factors such as polygamy practice of male dominance in marriage etc. affect the distribution of the Diseases.
Non specific genital infection is the commonest condition encountered, being responsible for 38. 86% of the cases. This agrees with studies from Jos, Zaria, Ibadan, and Lagos (12, 13, 14, and 15). Of the genital ulcerations, chancriod was most frequently encountered 9.02%. Chancroid is associated with hard sexual intercourse and unhygienic condition. There two factors are common features in this environment. In Jos and Lagos they recorded syphilis and herpes genitalis as the commonest of the genital ulcers 3.4 % and 6% respectively.
It was also observed that some patients use laboratory results as a shopping list for drugs instead of being used as a guide by Doctors for proper prescription.
The practice of reporting normal skin flora staphylococcus aureus only misinform clinicians and also encourage patient to buy inappropriate and most often dangerous drugs.
We conclude by suggesting that more should be done on health education of the people, the danger of self medications and use of antibiotics. Safe sex and abstinence from sex before marriage should be encourage in the community.
Acknowledgement
We are grateful to the authorities of Federal Medical Centre, Makurdi, General Hospital Otukpo and Marian Specialist Clinic for their support, in this research work.