Oncocytic Carcinoma of Minor Salivary Gland
H Singh, A Dhull, M Gill
Keywords
oncocytic carcinoma, salivary gland neoplasm
Citation
H Singh, A Dhull, M Gill. Oncocytic Carcinoma of Minor Salivary Gland. The Internet Journal of Third World Medicine. 2009 Volume 9 Number 1.
Abstract
Oncocytic neoplasms are tumors composed of epithelial cells with a large, granular cytoplasm that is rich in mitochondria. Oncocytic carcinomas are extremely uncommon neoplasms which occur predominantly in major salivary glands particularly the parotid. Oncocytic carcinoma arising from minor salivary gland is a rare entity. Management and prognosis of oncocytic carcinomas is not well established due to their low incidence. We report a case of oncocytic carcinoma of the minor salivary gland of lower lip.
Introduction
Oncocytes are large, granular, eosinophilic epithelial cells mainly found in glandular tissue, including that of the salivary glands and thyroid.1 Oncocytic neoplasms are tumors composed of epithelial cells with a large, granular cytoplasm that is rich in mitochondria.2 Oncocytic carcinomas are extremely uncommon neoplasms representing 0.18% of all epithelial salivary gland tumors.3 Oncocytic carcinoma was first reported in 1953 by Bauer and Bauer4. These predominantly occur in major salivary glands particularly the parotid.1, 2 Only a few cases of oncocytic carcinomas involving minor salivary gland have been reported in literature. We present such a case of oncocytic carcinoma involving minor salivary gland of the lower lip.
Case Report
A 60 year-old female was presented in the Radiotherapy Department with a painless lump over the lower lip of two months duration. The lesion initially developed as a whitish patch over the lower lip and rapidly increased in size within a month before presentation. Local examination revealed a pedunculated lump of size 5 x 4 cm over the lower lip in the midline. No lymph nodes were palpable. The skin over the mass was ulcerated. Fine needle aspiration cytology (FNAC) was suggestive of salivary gland neoplasm of uncertain biological behaviour. Excision of the mass was done with adequate margins. The histopathology revealed oncocytic carcinoma of minor salivary gland origin (Fig. 1&2).
Figure 1
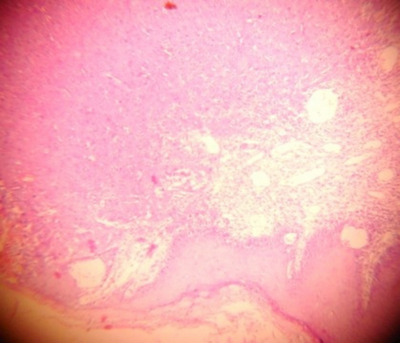
Figure 2

The patient was advised to undergo postoperative radiotherapy. The patient did not take any radiotherapy and reported after 4 months of surgery with cervical and axillary mass. Examination revealed an immobile right axillary lymph node of size 6 x 5 cm and bilateral cervical lymph nodes of 12 x 8 cm in size. FNAC from neck and axillary lymph node revealed metastasis from salivary gland neoplasm resembling the primary tumor (Fig. 3).
Figure 3

There was no evidence of metastasis on Chest X-ray examination and ultrasonography of the abdomen. The patient was given palliative radiotherapy to neck and axillary lymph nodes but showed no response to radiation after 6 weeks of treatment. The patient was planned for systemic chemotherapy which could not be given as she developed pleural effusion and her condition deteriorated. The patient was given symptomatic and supportive care.
Discussion
The salivary glands consist of the three large, paired major glands—parotid, submandibular, and sublingual and many smaller, minor glands distributed widely throughout the upper aerodigestive tract.5
Salivary gland malignancies make up only approximately 0.4% of all cancers represent for less than 5% of all head and neck tumors. Most salivary gland neoplasms occur between third to fifth decades. Benign tumors have a slight female predominance, but malignant tumors exhibit an equal sex distribution.5 Within the oral cavity most of the tumors occur in the palate (mostly the hard palate). In one series of labial minor salivary gland tumors, 85% of the tumors were reported from the upper lip and 15% were from the lower lip. Of the upper lip lesions only 10% were malignant, while in the lower lip 98.3% lesions were malignant. Other malignant epithelial neoplasms reported in the minor salivary glands include adenosquamous, epithelial-myoepithelial cell carcinoma, cell carcinoma, oncocytic carcinoma, squamous cell carcinoma, and undifferentiated carcinoma.6
Oncocytes are eosinophylic granular swollen cells in the human salivary glands, pharynx, trachea and esophagus. Oncocytic cells can also be seen in oncocytoma, Warthin’s tumor, metastatic renal and thyroid cancers, pleomorphic adenoma focally, acinic cell carcinoma, mucoepidermoid carcinoma and polymorphous low grade adenocarcinoma and non-neoplastic conditions such as oncocytic metaplasia and nodular oncocytic hyperplasia. Oncocytic carcinoma is a malignant epithelial salivary gland tumor characterized by oncocytes.2
Management of oncocytic carcinomas is not well established due to their low incidence. Treatment of oncocytic carcinomas consists of surgical intervention and radiotherapy, although the role of radiation therapy is not clear. Radiation does not appear to favourably alter the biological behavior of this tumor.4 Role of chemotherapy is also not well defined but cisplatin and fluorouracil have been used. The prognosis of oncocytic carcinomas is also not well known because of their low incidence. Distant metastasis though rare appears to be the most important prognostic feature of oncocytic carcinoma; local lymph node metastasis is not necessarily a critical factor in the overall prognosis.4 Tumors smaller than 2 cm diameter are associated with a good prognosis.7 An adequate neck dissection is mandatory only when nodal metastases and/or a nodal recurrence is present.2
Conclusion
Oncocytic carcinoma of minor salivary gland is an extremely rare tumor. Surgery is the mainstay of treatment however adjuvant treatment may be necessary depending upon the prognostic factors. Patients with poor prognostic factors should be aggressively treated.