A Review On The Prevalence Of Disabilities In Children
J Merrick, E Carmeli
Citation
J Merrick, E Carmeli. A Review On The Prevalence Of Disabilities In Children. The Internet Journal of Pediatrics and Neonatology. 2003 Volume 4 Number 1.
Abstract
Background: The definition of childhood disability has been defined and measured differently over time. There are various reasons for this distinction, ranging from the period of time in which the study took place, the attitude of society towards the disabled, the researcher and the purpose of the study. The World Health Organization has endeavored to classify disability, but there seems to be a need for further international guidelines on definition and study design.
Methods: This review looks at studies from the United Kingdom, United States, Denmark, Finland, Norway, Sweden, Iceland and Israel in order to find trends and common denominators in the prevalence of disability in childhood.
Results: The prevalence of children and adolescents with a disability in recent studies from Scandinavia, Israel and United States demonstrated the lowest rates in the United States ( 5.8%) and the highest in Finland (9.8%).
Conclusion: In spite of many differences in definition and study design, it appears that disability in childhood effects many children and adolescents in each country. There also seem to be an increase in the number of children surviving childhood with diseases or conditions that once were considered life-threatening. This emphasises the need for better coordinated service programs for that population. A transition to later adult health care is a problem that needs to be overcome.
Introduction
Childhood disabilities have been defined and measured differently depending on the purpose, the need, the researcher, the time and the attitude of the society where the study has taken place. Different terms have been used, such as chronic illness, chronic conditions, handicap, developmental disability, impairment or disabling chronic condition. Another problem is that a chronic condition in a child does not always result in disability and that disability may change over time.
Disability is a dynamic concept that varies in each individual depending on the context and the resources available. The World Health Organization (WHO) (1) has tried to classify the consequences of illness at three levels (International Classification of Impairments, Disabilities and Handicaps or ICIDH):
A uniform definition or classification has yet to be used by service providers (medical, educational, social welfare or rehabilitation services), researchers or policymakers. This creates diffculties in studying the scope of disability in childhood and is why such varied prevalence figures, ranging from 5-20%, are reported in English, American and Scandinavian literature (2).
After nearly twenty years experience with the ICIDH, the WHO published a revised version called the International Classification of Functioning, Disability and Health (ICF for short) in 2001 (3). This new classification instrument is complementary to the ICD-10 (International statistical classification of diseases and related health problems) (4), which classifies health conditions, diseases and disorders. The ICF goes beyond medical perspectives and includes societal and environmental perspectives in order to provide a scientific basis for understanding and studying health and health related states, outcomes and determinants. It was created to establish a common language for describing health and health related states, to permit comparison of data across countries and to provide a systematic coding scheme for health information systems (3). It is hoped that it will be used in the field more extensively over the coming years.
In recent years there have been discussions about the prevalence of disability in childhood in Israel. The purpose of this review was to examine different studies from around to world, over time, in order to form a more realistic picture of the prevalence and magnitude of disability during childhood. This data is compared to the current situation in Israel.
Methods
Israel has similarities with other countries. It is a small country with a welfare system similar to Scandinavia, a national health system like that in the United Kingdom and in many other ways closely linked to the United States. A Medline search was conducted using “disability prevalence and children” for United Kingdom (116 references found), United States (292 found), Scandinavia (79 found) and Israel (19 found). Our personal reference library was also utilized and relevant sources from both searches concerned with disability prevalence in childhood were used for this review.
Studies from the United Kingdom
The British Cohort Studies consists of data collected about the lives of close to 40,000 persons across three post-world-war generations - people born in one week of 1946 (called MRC National Survey of Health and Development- 1946), 1958 (called National Child Development Study-NCDS) and 1970 (called British Cohort Study-BCS70).
Data collections on the 1946 cohort were undertaken on the whole cohort at birth and then at ages 2, 4, 6, 7, 8, 9, 10, 11, 13, 15, 19, 20, 22, 23, 25, 26, 31, 36 and 43 years, on women at ages 47, 48, 49, 50 and 52 years, and firstborn children at ages 4 and 8 years.
A random sample of 5,362 children out of the 16,695 children from the MRC National Survey of Health and Development born in England, Wales and Scotland in the first week of March 1946 (3-9 March) (5) was selected for follow-up in 1961, when the children were 15 years old. Only 4,724 remained due to death, immigration or a refusal to participate. Over 15 years a variety of information on health, growth, development, behavior and education was collected from interviews with mothers, examination by school physicians, tests at different ages, ratings given by teachers at different ages and questionnaires filled out by the children at different ages.
Chronic illness in this study was defined as a physical, usually non-fatal condition, which lasted longer than three months in a given year or in need of continuous hospitalization of more than one month. In addition, conditions were only included if they were of sufficient severity to interfere with the ordinary activity of the child.
It was found that 528 children (224 girls and 304 boys) had one or more chronic physical disorders. This was a total prevalence of 112 per thousand under the age of 16 years or about 11 % of the population at risk (see Table 1). The 528 children with a disability were compared to the rest of the cohort and it was found that there was a significantly higher proportion of boys than girls in the disability group. The social class, family size or father's health did not seem to show any difference. The mothers of children with a disability were significantly more often described as being in fair or poor health compared with the control group.
Figure 1

At age 15 the status of the children was reviewed and 60 % of the conditions of disability were still present. The disorders were rated as follows: 54 % mild disabilities, 34 % moderate and 12 % severe (5).
The National Child Development Study (NCDS) is also a continuing, multi-disciplinary longitudinal study with persons living in Great Britain and born between 3 and 9 March, 1958. Following the initial birth survey in 1958 - the Perinatal Mortality Survey (PMS) - there have been, to date, five attempts to trace all members of the birth cohort in order to monitor their physical, educational, social and economic development. These were carried out by the National Children's Bureau in 1965 (NCDS1), 1969 (NCDS2), 1974 (NCDS3) and 1981 (NCDS4); and by the Centre for Longitudinal Studies (CLS), Institute of Education (formerly the Social Statistics Research Unit, City University) in 1991 (NCDS5). In addition, in 1978, details of public examination entry and performance where obtained from schools and colleges. NCDS data are available for secondary analysis from The Data Archive at the University of Essex, and on-line at MIMAS (Manchester Info-Mation and Associated Services) (6).
This 1958 cohort showed disability rate of 5.15% at age 7 years (739/14,627), 9.6% at age 16 years (1,249/13,041) and the prevalence of longstanding limiting illness at age 23 years was 5.1% for men and 4.1% for women, which increased to 6% at age 23 years for both sexes (7).
The famous study performed on the Isle of Wight (8) among 10-12 year old children (total 3,271 children) found an overall disability rate of 56.6 per 1000 with a rate per 1000 of 16.4 for respiratory, 17.8 for neurological, 3.0 for sensory, 2.4 for musculoskeletal, 1.5 for congenital, 6.4 for dermatological, 1.2 for genitourinary and 7.9 for miscellaneous diseases.
Another study method was used by Weale and Bradshaw (9) with the 1974 General Household Survey, where they found that 7.6% of children under 16 years of age had a long standing illness, disability or infirmity. 10% were classified as severe, 29% moderate and 61% mild.
Studies from the United States
The now classic Rochester Child Health Survey conducted in 1967, 1969 and 1971 in Monroe County, New York (10,11) consisted of a one percent probability sample of all children under 18 years of age (1.756 children). Parents were first questioned about their children's health and based on the replies a group of children of school age with symptoms of chronic illnesses and a matched control group was selected for intensive study.
Of the more than 1,700 children initially studied, 350 were described as having symptoms of chronic physical disorders considered by their parents to be serious. Of the 350 described by parents, 206 were confirmed later by the research team.
The overall disability rate was found to be 118.8 per 1000 with a rate of 45.6 for respiratory, 8.5 for neurological, 23.9 for sensory, 4.0 for musculoskeletal, 2.8 for congenital, 15.9 for dermatological, 5.7 for genitourinary, 1.7 for hematologic and 5.1 for miscellaneous diseases.
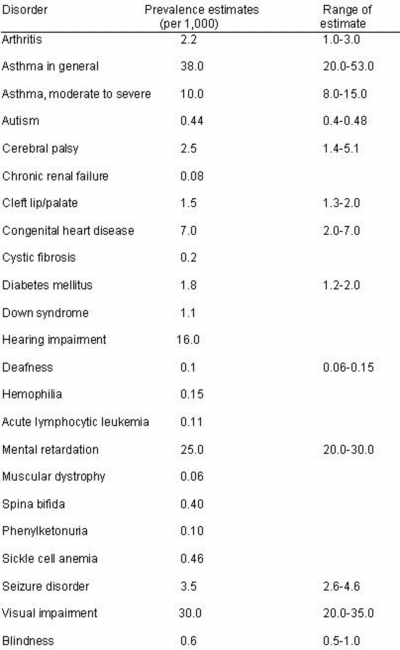
In a review of several studies, researchers from Harvard School of Public Health estimated the prevalence of various chronic diseases in children and adolescents in the United States in 1980 (12). The results are shown in Table 2. The authors cautioned than the data upon was based on data of varied quality and did not estimate the overall disability rate.
Figure 2
Researchers from the Institute for Health Policy in San Francisco have been very active in analyzing National Health Surveys. Among 15,181 randomly selected adolescents (aged 10-18 years) in 1984 it was found that 6% (or 1.4 million adolescents) suffered some degree of disability or limitation (13) in their daily activity. Adolescents living in poverty and in households with little formal parental education had increased risk of disability. The disabled adolescents had three times as many physician contacts annually and nine times as many days hospitalized as their non-disabled counterparts.
In a 1988 sample of 7465 adolescents aged 10-17 years from the National Health Interview Survey on Child Health (14) it was found that 31.5% of the adolescents had one or more chronic conditions. Respiratory allergy was found in 9.7 per 100, repeated ear infection in 8.3 per 100 and asthma in 4.3 per 100. Of the adolescent with disability 66% had a mild condition with little or no limitation in activity, 29% had moderate severity and 5% severe limitation. The adolescents with severe limitations accounted for 19% of physician contacts and 33% of hospital days related to chronic illness (15).
Results from the 1994 National Health Interview Survey on Disability among 30,032 children and adolescents under 18 years of age revealed that 18% had a chronic physical, developmental, behavioral or emotional condition that required health and related services of a type and amount beyond that required by children in general (16).
The Division of Birth Defects and Developmental Disabilities of the Centers for Disease Control have studied the prevalence of developmental disabilities in 10 year old children from five counties in Georgia during 1985-88. The rate of mental retardation was 10.3 (1.03%), cerebral palsy 2.0 (0.2%), visual impairment 0.6 (0.06%) and hearing impairment 1.0 (0.1%) per 1000 ten year old children (17).
A new birth cohort study sponsored by the U.S. Department of Education, National Center for Education Statistics (NCES) in collaboration with the National Center for Health Statistics (NCHS), the National Institutes for Child Health and Human Development (NICHD), the National Institutes of Health (NIH), the Administration for Children, Youth, and Families (ACYF), and the U.S. Department of Agriculture has been undertaken in the year 2000. This will be a nationally representative sample of 15,000 children born in the calendar year 2000 and followed longitudinally from birth through to the end of first grade. The sampled children will come from diverse racial-ethnic and socioeconomic backgrounds (18). It is hoped that this study will also look at childhood disability and that the study will continue after first grade.
Studies from Scandinavia
In Denmark, the Copenhagen Perinatal Birth Cohort (19) was initiated in 1959-61. It consisted of 9,006 pregnant women (9,125 successive live births) and the children are still followed to this day. Of the 8,425 children, who survived beyond 28 days of life, school health records were traced for 4,327 (51.4 %) and evaluated (20) finding that 484 had a disability diagnosis corresponding to 11.2 % of the records evaluated.
As a result of the experience with the Copenhagen Perinatal Birth Cohort a much larger study was initiated in 1997 (21) with data collection on pregnancy ending in 2002. This study will be a longitudinal study of 100,000 pregnant women and their children and the largest pregnancy cohort undertaken. Information on disability will surely emerge from this study.
In Sweden in 1975 (22) an epidemiological study of school children and a follow-up of previous health care was conducted in a group of 223 ten year old children. Health problems of importance for the day-to-day functioning of the child were the target of the study. Overall 26.1% significant deviations were found. Physical disorders comprised 11.7 %, visual defects 11.7% and auditory impairment was found in 2.7%. The vast majority of the health problems were already known to the parent and physician, but in 4.4% a new health problem was detected by the examination. By the physical examination 0.9% of the new problems were detected, 2.6% by vision screening and 0.9% by auditory screening. The most frequent health problem was allergy (13.5%).
In Finland in the 1970s several studies reported a frequency of long-term illness in children of between 1.4-9.6% (2) and in Norway parents reported in 1975 that 12% of pre-school children and 14.9% of children aged 7-15 years had some form of chronic illness with a duration of at leat six months. Data from Iceland was not available for the 1970s.
Due to the differences and quality of various Scandinavian studies, the Nordic School of Public Health in Gothenburg (Sweden) decided to conduct several studies of child health and well-being in Scandinavia (Sweden, Denmark, Norway, Finland and Iceland). One study of 10,475 randomly sampled children in 1984-85 (2,23) and another of 10,664 children in 1996 (24) was carried out by research teams in each Nordic country and coordinated by the principal investigator in Gothenburg. The studies were conducted as a questionnaire study with over 3,000 contacts in each country and a response rate of 56-83 %. In the 1984-85 study, chronic illness or handicap was defined as a condition, which for at least three months had seriously affected the daily life of the child, during the last year. The data for disability is shown in table 3. A total of 7.9 % of the 10,475 children had a disability, with 7.4 % for girls, 8.3 for boys and increasing with older age. In the adolescent group 8.5 % had a disability.
Figure 3

Studies from Israel
The Jerusalem Perinatal Study, a research database with information on fetal and maternal outcomes on 92,000 births in 1964-76 has unfortunately not been interested in childhood disability and to our knowledge has not published on this subject.
A study of 9,492 Jewish 2-3 years old born in 1980 was conducted in 1983 based on records from Family Health Centers (25). In this time period 95 % of all children born in Israel attended Family Health Centers regularly with an average of 17 visits during the first two years of life. The sample was 13 % of the National Jewish birth cohort of 1980 (total 71,372) and came from 118 out of the 870 Family Health Centers in operation at the time. Data was collected from 9,349 files at the centers and from 143 hospital files of children who had died.
Disability was defined as “children who have special needs for health and other services in comparison with their peers, due to their health condition”. An expert team defined 76 health conditions causing disability and categorized them in 16 groups based on the International Classification of Disease (ICD). In this cohort 8,499 (89 %) children were found to be healthy, 845 (8.9 %) had at least one disability and 148 (1.6 %) had died. The total number of disabilities found was 1,329 for the 845 children corresponding to 1.6 conditions per child. The male:female ratio ranged from 1.4 to 2.1.
Another study by the same research team (26) looked at the birth cohort of Jewish children born in 1975, who had reached the age of 7 years in 1982. The study was based on a sample of records from 150 mainstream schools (6,969 children in fourth grade corresponding to 10.2 %) and 770 children (100 %) from the fourth grade in special schools.
Of the 6,969 children from the mainstream schools, 1,219 or 17.5 % had at least one disability. The total number of conditions recorded was 2,136 or 0.31 per child. In the special education group, 100 % of the children had at least one disability. Of the 770 children in special education, 1,821 diagnoses were recorded or 2.4 disabilities per child. As before, boys featured more than girls.
During 1995-98 the JDC-Brookdale Institute and the National Insurance Institute conducted a National study of 5,691 households in Israel, with 13,453 children aged 0-18 years. This included 10,993 Jewish children, 236 Arab children in joint Jewish-Arab towns and 2,224 children from Arab villages (27).
The study was conducted through telephone interviews or home visits with a particularly high response rate (97.2%). The total disability rate was found to be 12.8 %. Of these, 3.6% suffered from a chronic handicap (e.g. asthma) that did not affect the functioning of the child or needed daily treatment. 0.8 % suffered from a temporary problem and 0.7 % suffered from a chronic illness, but received medical treatment only periodically (e.g. decreased hearing on one ear only).
This leaves a total 7.7% of the children with a chronic disability that required continued care for more than one year. The number of boys with special needs is nearly double that of girls: 9.8 % versus 5.4 % and the proportion in different age groups were 5.2 % in the 0-5 year olds, 10.7 % in the 6-11 year olds and 7.0 % in the 12-18 year olds. These figures are compared with Scandinavia in Table 3. Both the Scandinavian and Israeli studies did not include children in boarding schools or institutions, which would make the estimate a little higher.
Discussion
Research on disability in childhood and its prevalence is of importance to every country in order to provide a sound basis for the determination and planning of service needs.
The United Nations have an international database on the prevalence rates of disability in childhood from 55 countries around the world (28). These disability rates are from different national surveys conducted from the years 1975-84. When a comparison is undertaken it becomes very problematic due to difference in definition and populations studied. There is also variations in which segment of the population the studies have taken place. Some cover all children, others only older children and some are only representative of certain segments of the population (for example rural or urban children). The findings from 55 countries showed the lowest disability rate in Burma (1.1 per 1,000 children under the age of 15 years) and the highest in Canada (56.7). The difference in the rates might be due to the use of functional definition of disability as opposed to a categorical definition or more advanced survey methods or cultural differences on how disability is viewed or recognized (28). The data from this database suggests an urgent need for a more standard method to measure disability rates.
Reviewing research studies from United Kingdom, United States, Scandinavia and Israel revealed a need to examine not only the total disability rate, but also categorize the disability into mild, moderate and severe, because a child or adolescent with mild asthma without any restriction in daily activity should be in the category of mild disability. This categorization was not found in all the studies, but should be considered in future studies, just as future studies should take into account the new WHO classification of functioning, disability and health (3).
Practical aspects
Due to the increase in survival of children with once life-threatening conditions, the practising physician will encounter more children and adolescents with complex chronic illnesses that will require continuous service and transition from pediatric/adolescent health care to adult health care service (29). A recent survey of programs in United States (29) revealed the lack of a coherent system to allow such a transition. The transition process was evident in health services, where the following elements were in place: a) professional and environmental or institutional support; b) decision-making and consent; c) family support and d) professional sensitivity to the psychosocial issues of disability. The study also indicated that self-identified transitional health care programs are not, in general, providing collaborative, coordinated and integrative services to adolescents with chronic or disabling conditions. It appears that the barriers to obtaining this goal are not the adolescent or their parents, but rather limitations of the health care system itself.
Conclusion
This review looked at studies on the prevalence of disability in childhood and adolescence in order to find common trends. In spite of many differences in definition and study design it seems that disability in childhood effects a considerable number of children and adolescents in each country.
There also seem to be an increase in the number of children surviving childhood with diseases or conditions that once were considered life-threatening resulting in a need for better coordinated service programs for that population. A transition to later adult health care seems to be a problem, at least in the United States (29).
The prevalence of children and adolescents with a disability in recent studies from Scandinavia, Israel) and United States showed the lowest rate of 5.8% in the United States and the highest in Finland (9.8%).