Poverty, Children And Families In Israel: A Public Health Concern
J Merrick, M Morad, E Carmeli
Citation
J Merrick, M Morad, E Carmeli. Poverty, Children And Families In Israel: A Public Health Concern. The Internet Journal of Pediatrics and Neonatology. 2002 Volume 3 Number 1.
Abstract
Background: Several studies from Europe have over time shown that children growing up in poverty will have long lasting effects on their physical and mental health, on medical service utilization, and criminal behavior. Poverty exists even in developed countries such as the United States and Israel (25% of children living in poverty), where it is a major public health problem of a magnitude that is markedly different than Scandinavian countries (3%).
Methods: This paper presents data from the Israel National Insurance Institute research on poverty, with comparisons with several other countries.
Results: The data showed the incidence of poverty in Israel at 18% of all families. The number of families living in poverty in 2000 was 305,400 with 1,088,100 persons and 481,100 children. In other words 25% of the children or every fourth child in Israel live in poverty.
Conclusions: It is concluded that there is a need for further research into the effects of poverty on child development and adaptive behaviors, and to find ways to conduct policy relevant research. Pediatricians and child health care workers should also be trained in community advocacy work in order to work as a coalition in the community towards prevention of poverty and poverty related health problems.
Introduction
A now famous study was conducted in inner London in 1896 by Charles Booth. His work on poverty was published between 1889 and 1903 in 17 volumes under the title “Life and labour of the people of London” 1. His original survey covered over 120,000 households and resulted in the construction of detailed and exact maps of the poverty in London. A research group of scholars from the School of Geography at the Universities of Leeds, Bristol and Cardiff (1) took the data from the 1896 study of Booth and compared it with the findings of the 1991 United Kingdom census of the population. All deaths in the area between 1991-95 were identified and standarised mortality rates for various causes of death were calculated for all ages, under age 65 years and above.
They found that for many causes of death in London, measures of deprivation made around 1896 and 1991 both contributed strongly to predicting distribution. The present mortality from diseases known to be related to deprivation in early life (stomach cancer, stroke, lung cancer) was predicted more strongly by the distribution of poverty in 1896 than in 1991. Mortality of older persons (above 65 years) was slightly more strongly related to poverty in 1896 than to its present distrubution. This present day study showed that today's patterns of diseases have strong historical roots and the fundamental relation between spatial patterns of social deprivation and spatial patterns of mortality is so strong that a 100 year difference in time did not make a big difference 1.
A study published in Denmark in 1956 2 looked at all incidences of hospitalizations for children aged 0-7 years for the period 1948-52 from different housing condition areas of Copenhagen. Thirty years later these children (original sample 2,982 children) were followed and it turned out that unfavourable housing conditions during childhood was not only a powerful predictor for later occurrence of somatic and psychiatric illness, but also for conviction of criminal offences. Compared to the general population these children from the slum areas had nine times more hospitalization for suicide, five times more for psychiatric hospitalization, three times more hospitalization for somatic disease, eight times more arrests for delinquency and five times more convictions 3.
In the United States the official poverty rate for children declined sharply between 1960-69 but had an upward trend between 1969-93 with a steady figure of around 20% since 1981. In 1996, the federal government counted 20.5% of the children poor, 18.3% of those 6-17 years of age and 22.7% of all those under six years of age. In 1996, 16.3% of all White children were living in poverty, 39.9% of all Black children and 40.3% of all Hispanic children 4.
The last Unicef report on child poverty in rich nations showed that one in six children today live in relative poverty (below the national poverty line in their country) with the United Kingdom, Italy, the United States and Mexico in the lower end of the scale of 23 rich countries and Sweden, Norway, Finland, Belgium, Luxembourg and Denmark in the upper scale with a child poverty rate of about 5%. This rate has been constant in the last twenty years for the Nordic countries 5.
The purpose of this review was to look at the data available on poverty in Israel, related to children and families and to compare these findings with other countries.
Data On Poverty In Israel
The National Insurance Institute in Israel has over the years carried out research on poverty by processing data from the Central Bureau of Statistics Income Surveys 6,7 , which we reviewed and analysed.
The methods to measure poverty in Israel are based on three factors. The
The poverty line per standard person in Israel was set at 50% of the median net income per standard person and a family in Israel was considered poor, if its net income, divided by the number of standard persons in the family was lower than the poverty line per standard person. The poverty line per family can be calculated by multiplying the poverty line per standard person by the number of standard persons in the family 6.
From 1998 the Central Bureau of Statistics has produced a combined Income Survey, based on both the current Income Survey and the Family Expenditure Survey. This combined Survey encompasses 95% of all households in Israel in most forms of settlements.
The poverty incidence reflects the scope of poverty by giving the percentage of poor families in the total population and the poverty gap indicates the depth of poverty. The poverty gap index or ratio can be standarized and defined as the ratio between the average poverty gap per poor family and the poverty line. The income inequality among the entire population is measured by the GINI index6,7 .
Results From The Combined Income Surveys In Israel In Recent Years
The data from 1998, 1999 and 2000 is shown in Table 1. Over this three year period the incidence of poverty was constant with around 18% of all families. The number of families living in poverty in 2000 was 305,400 with 1,088,100 persons and 481,100 children. In other words 25% of the children or every fourth child in Israel live in poverty.
Figure 1

Figure 2

The incidence of poverty among families headed by an elderly person rose from 24.3% in 1998 to 25% in 1999 6, which was caused by the slight erosion in the level of the basic old-age pension, but came back to 24.4 in 2000 7. The incidence of poverty among families with children increased from 17.9% in 1998 to 19.3% in 1999 6, which was mainly caused by the rise in poverty among large families with four or more children. However, it rose dramatically to 32.7% in 2000 7. In 1999 the net income in 41.6% of large families was below the poverty line. The incidence of poverty among large Jewish families did not change significantly, but among large non-Jewish families it rose from 50% in 1998 to 61% in 1999 due to a rise in unemployment 6.
The incidence of poverty in 1999 in families headed by a working person was at the same level as 1998 (9.3%) with the same trend for families headed by a non-worker (at 62%)6, but in 2000 it fell to 9.0% for workers and stayed at 62.4% for non-workers 7. In single parent families the rate was 23.7% in 1999 6 and 25.1% in 2000 7 and in non-Jewish families 42.3% in 1999 6 and 42.9% in 2000 7. The incidence in new immigrant families rose from 16.8% in 1998 to 18.0% in 1999 6 and to 18.7% in 2000 7.
There were marked differences in the distribution of poverty, when the map of Israel was studied in 2000 7 . The Jerusalem district, the northern district and the southern district were all with a high incidence of poverty with 29% in the north, 23.3% in Jerusalem and 20% in the south. The poorest cities in Israel were Jerusalem, Bnei Brak and Ashdod with 22-33% of the families below the poverty line. 7
The income gap in Israel became worse from 1997 to 1999, when the GINI index rose from 0.509 to 0.512 6, but it decreased to 0.509 again in 2000 7.
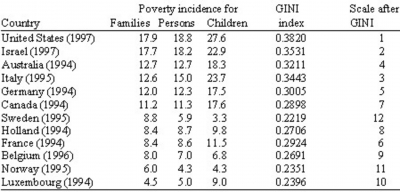
Israel Compared To Other Countries
When Israel was compared to some other developed countries (see Table 2) it was found that only United States had a worse poverty incidence with Sweden, Norway and Luxembourg at the better end of the scale. The children of Scandinavia came out with the lowest percentage in the 3-4% range.
Figure 3
The
Poverty And Health
The studies from England1 and Denmark 2,3 showed marked long term health effects on growing up in poor neighbourhoods. Other studies 9 have also shown adverse effects on child development and health when growing up in poverty. When living in poverty, children will have less access to optimal medical care and surveillance, proper nutrition and safe environments.
The health problems will often persist and have consequences for long-term development 1,2 3,9.
Discussion
In recent years there has been some discussion10 about the definition of poverty and what it measures. The US Government will consider a family poor, when its pre-taxation cash income falls below the standard poverty line4. The poverty line is adjusted each year by inflation according to the minimal amount of money that is needed to maintain a nutritionally adequate diet for different family size and composition.
In 1996 the US Government found 20.5% of its children poor4, while the 1999 results from the Combined Income Survey in Israel showed a certain degree of deterioration compared with earlier years in aspects of the scope of poverty, income gaps and more children living in poverty (26%). The statistics both from the US and Israel do not however show to which degree each family is economically disadvantaged, the length of poverty time for each family or child and at what point in development time each child is affected.
Poverty can have serious effects on child development and health9,11 and is often associated with other risk factors, such as low birthweight, single parenthood, unemployment, unsafe neighborhoods, maternal depression, low social support, welfare dependence and stressful life events 9. Poverty means less or even lack of medical services, which will influence the child from the foetal stage. Mothers living in poverty will not be able to get the right nutrition during pregnancy, will not receive proper antenatal care and as a result have a higher incidence of low birthweight babies, higher infant mortality and therefore a higher risk for permanent neurological or developmental impairment 9,11.
Growing up in poverty with inadequate living conditions, poor health service and poor nutrition will effect the development of the child, the performance in school and the health status, sometimes resulting in permanent damage that effects the quality of life and the lack of equal opportunity. Three recent publications from the
A recent comment in the
Children and adolsecents should be seen as a defined and specific client group in all hierachies of responsibilities
An independent children's commissioner or ombudsman for England working with others in Scotland, Wales and Northern Ireland should be responsible for integrating and evaluating the impact of all threads of government policy that relate to children and adolescents and for protecting their rights
A national strategy for children's and young people's health should be informed by multiprofessional strategic forums that have direct access to the management executive, chief medical officer and chief nurse and implemented by designated officials with identified responsibilities for children
Individuals should be appointed at regional, district and trust level to be responsible for defining local health policy, priorities and practices relating to children and adolescents. This is particularly important to ensure that the opportunities provided by the development of primary care groups and trusts are not compromised by the creation of a new functional barriers between service providers
Authority should be given to implement change and to deliver effective services in the light of specific budgets for children and adolescents and their health needs within the framework of local health improvement programmes for young people
Children's health imrpovement programmes should be truly intersectorial embracing other joint children's planning devices, paryicularly children's and young people's services plans
Local multiprofessional forums between education, social services and health should be created to inform strategy, monitor performance nd develop joint commissioning
Effectice leadership is needed at all levels to facilitate jointed up working with effective intersectorial communication, collaboration and working practices
The views of parents, children and adolescents together with those of clinicians dealing with young people urgently need to be incorporated into the formulation of strategy and delivery of services
The authors claimed that the government in the United Kingdom has failed to monitor the implementation of existing guidance despite several reports and committees showing that some of the basic principles in the health care of children are ignored.
There is therefore a need for physicians working with children and adolescents to embark upon the task of not only dealing with ailments and health, but also to become advocates for children and young people's rights.
The late pediatrician
Conclusions
Living and growing up in poverty places children and adolescents at risk for developing health problems due to inadequate health care, health insurance, inproper nutrition and sometimes hazardous living environments.
Research 9 has shown concern for the psychological effects on children living in poverty and there is a need for further research into the effects of poverty on child development, resiliency andadaptive behaviors. There is no good reason for the big difference in poverty between children living in Sweden or Scandinavia compared to United States and Israel.
Conflict of interest: None
Correspondence to
Professor Joav Merrick Email: jmerrick@aquanet.co.il