Aspiration of barium sulphate in swallow study
B Wani, M Yeola
Keywords
barium sulphate, barium swallow
Citation
B Wani, M Yeola. Aspiration of barium sulphate in swallow study. The Internet Journal of Pulmonary Medicine. 2008 Volume 10 Number 2.
Abstract
Barium swallow is the simple, common routine procedure for the examination of the oropharynx and oesophagus. Aspiration of barium sulphate is a well known complication, occurs accidentally during contrast enhanced examinations of the upper gastrointestinal system. It is reported either as rare or frequent, based on severity of the cases. Certain conditions affecting the anatomical and functional integrity of the oropharynx and oesophagus act as predisposing factors Due to relatively non-irritant nature of barium sulphate, aspiration into the lungs not expected to cause severe lung injury. However, acute inflammation or even death due to high or low density preparations of barium sulphate, have been reported. We present a case of dysphagia, who developed aspiration of barium, during swallow study and managed conservatively without any delayed complications.
Introduction
Barium swallow is the simplest, common routine procedure for the examination of the oropharynx and oesophagus. Barium sulphate is insoluble salt of barium used as a radiographic contrast medium. [1] Rarely some amount of barium sulphate is accidentally aspirated into the lung during an upper-gastrointestinal radiographic contrast procedure. [2]
Case History
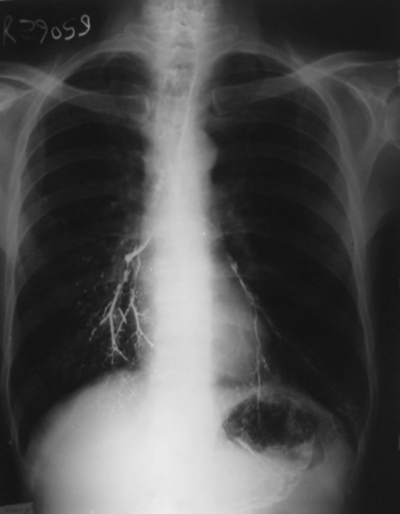
A 53 year old male patient, suffering from chronic dysphagia, underwent a barium swallow study with barium sulphate about 60 - 80 ml in standing position. The patient aspirated some amount of barium sulphate; had immediate cough and became dyspnoeic. Chest X-ray showed alveolar deposition of barium sulphate in the form of dense punctate foci, distributed to both lower lung lobes.
The patient managed conservatively requiring assisted ventilation and chest physiotherapy followed by oral antibiotics for seven days. The patient has recovered well after 24 hours and without any delayed complications.
Figure 1
Discussion
Aspiration of barium sulphate is a well known complication, occuring accidentally during contrast enhanced examinations of the upper gastrointestinal system. [2] The mortality rate associated with massive barium aspiration is approximately 30% and exceeds 50% in patients with initial shock or apnoea, secondary pneumonia, or adult respiratory distress syndrome. [3] Aspiration can occur in certain conditions involving the anatomical and functional integrity of the oropharyngeal and oesophageal segments, in the extremes of age, disordered swallowing, neuromuscular dysfunction, broncho-oesophageal fistula, alcoholism, head and neck cancer and psychological illness, and commonly associated with functional gastrointestinal disorders. [4,5,6,7] The basal segments of the lower lobes are commonly involved when the patient is in the erect position, while the middle lobe if the patient inclines forward, as during vomiting or coughing, and the posterior segments of the upper lobes or superior segments of the lower lobes in the recumbent position. [4, 6] Due to relatively non-irritant nature of barium sulphate, aspiration into the lungs not expected to cause severe lung injury. However, acute inflammation or even death due to high or low density preparations of barium sulphate, have been reported. [2, 4, 8] The volume of aspirated material plays an important role in the progression of aspiration, even if there are reports of lack of signs of lung injury in terms of neutrophil sequestration and oedema which is usually seen after acid aspiration. [9]
The pattern visible in X-ray or in lung CT may be time dependent, due to a slow progressive clearance of the barium particles. [5] The barium particles, not eliminated by coughing and the mucocilliary apparatus, accumulate in alveolar spaces or peribronchial interstitial tissue and become phagocytosed by alveolar macrophages leading to fibrosis. [5] Plain chest radiographs remain the method of choice in the acute phase, [6] while lung HRCT is indicated only in severe cases and is useful in evaluating long term prognosis. Differential diagnosis, where the history is not cleared, may include alveolar microlithiasis with similar paving pattern in the lower lobes, deposition of calcium within the lung due to hypercalcemia in patients with chronic renal failure and secondary hyperparathyroidism, pulmonary ossifications of various causes, hemosiderosis, amiodarone toxicity, silicosis and heavy metal pneumoconiosis. [5, 6] The treatment is based on common sense and clinical judgment as no prospective controlled trials on the treatment are available. In cases of hypoxemia and dyspnea after massive aspiration, bronchoscopy is recommended to eliminate as much barium as possible, and for microbiology testing. [1] Bronchoalveolar lavage is not recommended because of the danger of dissemination of the contrast medium into the bronchoalveolar system. In cases of a probable infection antibiotic treatments with anaerobic coverage should be initiated. [4] The early recognition of predisposing factors, pre-treatment with antireflux medications, such as domperidone, and correct choice of contrast media will help in prevention.
Conclusion
Complications of barium sulphate aspiration depend upon the density and quantity of the aspirated solution, the extent of tracheobronchial distribution and the general physical condition of the patient. In nonsymptomatic cases, like ours, early treatment and close follow up with chest physiotherapy are mandatory to prevent progression towards fibrosis. Apart from other factors predisposing to aspiration, particular caution should be taken when performing relevant procedures.