Traumatic Brain Injury; Case experience as a model for learning and literature review
A Ara, I Bhat
Citation
A Ara, I Bhat. Traumatic Brain Injury; Case experience as a model for learning and literature review. The Internet Journal of Health. 2009 Volume 10 Number 2.
Abstract
The history, evaluation, treatment and follow-up of a patient with Traumatic Brain Injury (TBI) are presented to illustrate the approach and the difficulties that may be encountered. The literature on TBI is reviewed and a checklist prepared that covers the historical aspects, evaluative procedures, and treatment approaches to TBI. The work with the illustrative case has been compared to the literature review check list to evaluate the completeness of the patient’s care. The result of attempts to obtain outside information, of events prior to the trauma, immediately after the trauma and concurrent with the ongoing treatment also are described. The value of proceeding from a textbook to reviews to recent articles is illustrated.
Introduction
A single case may be used as a springboard for learning about an illness. Case presentations and case based learning can be used as an opportunity for self learning. Moving from textbook to review articles and then to the current literature can elucidate different aspects of a case from evaluative process to management to recovery to successful discharge and finally to normal premorbid functioning if possible. Using this sequence will not only help in learning more about a particular condition but also consolidate what is already known. Case based learning may be very informative, instructive, educational and stimulating.
In this article, a case report of TBI with psychiatric manifestations has been used to illustrate the learning process. TBI is a condition that involves different specialties to coordinate the care of the patient. TBI is a major public health problem and is often accompanied by significant psychiatric manifestations1-3. More than 1.5 million people suffer from TBI annually and more than 50,000 die from it4-7. TBI costs the country more than $56 billion a year6, 8. TBI causes different kinds of psychiatric manifestations which include but are not limited to Cognitive Deficits9a, Mood Disorders9b, Anxiety Disorders9c, Psychosis9d, Apathy9e, 10, Behavioral9f or Dyscontrol Disorders9g, Sexual Dysfunction9h and Sleep Disturbances11.
The patient presented in this report was involved in an automobile accident and suffered TBI. This injury has left a huge impact on the life of this patient and serves as a vivid example of how describing the management of such a case can be used for learning purposes by comparing it with what is in the literature. An attempt has also been made to demonstrate from this single case presentation that actual medical practice does not always follow the clinical guidelines. This has been done by comparing the management of this case with the checklist that has been prepared from a review of the literature.
Study Method
The sequence of the literature review has been from textbook, to review articles to the current literature. A literature search using review articles and the current literature on the subject from 1990-2009 has been conducted and electronic databases including Medline and Ovid have been used for this purpose. The search has been done identifying articles with the two key phrases ‘Psychiatric Manifestations’ and ‘Traumatic Brain Injury’. The articles that have been selected are review articles and current literature on the subject. Patient records were obtained from a university teaching hospital and other hospitals after obtaining consent for the release of information from the patient. The literature search was conducted at the university hospital library. A checklist has been developed which has been used for comparison with the actual management of this case. A review of in-patient and out-patient records from the university hospital and outside has also been done. An attempt has been made to gather data about the patient, including the history of the accident, evaluation during the initial and subsequent hospitalizations, treatment, the reason for referral to psychiatry, the response to treatment and further testing. The results of attempts made to obtain information and the problems faced in getting the information have been presented as well. An independent interview was conducted with the patient. Further information was obtained from his mother and girlfriend. The patient underwent Neuropsychological evaluation in the psychiatry department.
The checklist, as described above, has been used to compare the evaluation, treatment and management of this case against the various standards of practice in the current medical literature. Two of the most widely used measures for assessing the outcome of patients with TBI, the Glasgow Outcome Scale (GOS)9i, 12-17 and the Disability Rating Scale (DRS)12, 13, 15, 54 have also been described briefly (see Appendices I and II). Institutional Review Board (IRB) approval was not required for this report.
Case Summary
A 29-year-old, right-handed white male was involved in a motor vehicle accident in 1995 when he was 16 years old. The patient was ejected from his car and then run over by an oncoming vehicle and dragged for some distance. He was in a coma for one month before regaining consciousness. He was an unrestrained driver when the accident occurred. He had experienced a tire blowout and hit a pothole and then a tree. The patient was thrown out a closed window on the driver’s side.
The patient’s Glasgow Coma Scale (GCS)9j, 18, 19 (see Appendix III) on arrival in the Emergency Room (ER) was 5 and he had a decerebrate posture. The patient underwent non-contrast CT scan of the head in the ER which revealed hyper-densities in the right temporal lobe and left temporal contusion. The study revealed scattered hemorrhagic contusions and evidence of a shearing injury through the parietal and occipital lobes. The ventricular system was compressed, consistent with diffuse brain edema.
No alcohol was detected in his urine or blood although marijuana was detected in the urine. A right frontal intracranial pressure (ICP) monitor was placed on the day of admission. The patient was transferred to the Neurological Intensive Care Unit (NICU). The patient was started on Mannitol and to maximize cerebral perfusion pressure hyperdymanic therapy was instituted. Cognitive status from initial assessment in the NICU was Rancho Level II (see Appendix IV) which subsequently progressed during the course of the hospitalization to Rancho Level +VI/-VII. The patient during the hospitalization had developed septicemia and pneumonia. The blood and sputum cultures on the fifth day of admission revealed a Staphylococcus aureus infection. The patient was put on Gentamycin, Phenytoin and subcutaneous Heparin. The patient underwent surgical procedures including tracheostomy with mechanical ventilation and jejunostomy (J-tube placement) for diminishing voluntary breathing and feeding purposes, respectively.
Subsequent CT scan showed mild diffuse cerebral atrophy, complete regression of the subdural effusions on the right side and considerable regression of the left subdural effusion with only a small subdural collection on the left side. The patient underwent Swallowing Function Fluoroscopy which was normal. The patient progressed to bladder and bowel continence about one and a half months after admission. After about one month, he was able to open his eyes. The patient recovered some form of speech one and a half months after admission. The patient participated in physical therapy after about one month following admission. The patient, during hospitalization and rehabilitation had episodes of agitation, delusion and occasional periods of disorientation to time and place and these episodes were treated with haloperidol on an as needed basis. The patient was weaned from his tracheostomy and mechanical ventilation as well as J-tube. He was started on oral feedings and tolerated a general diet with no restrictions. He was able to take all nutrition orally.
The patient’s motor control was impaired and an Electromyogram (EMG) during the hospitalization showed some weakness of the left shoulder girdle and incomplete left upper brachial plexopathy. Gait and mobility had progressed to moderate assistance and due to residual ataxia the patient was able walk using a rolling walker. Activities of Daily Living (ADLs) progressed to minimal assistance in the upper extremities and moderate assistance in the lower extremities. As self awareness improved, cognitively, the patient, close to the time of discharge still had some time confusion. Some frustration and depression was also noticed. There were incidents of occasional disorganized thinking and tangential and preservative features. The patient needed assistance for learning new skills. The patient also had problems with double vision.
The patient was discharged to a short-term cognitive rehabilitation service where patients with TBI are taught independent living. Details of this admission are not available. Three years later he went to a long-term cognitive rehabilitation service where he stayed there for 9 month. The patient received training in handling money, crossing streets and going out in the community during admissions to out-patient rehabilitation services.
The patient was referred for a neuropsychological evaluation in March 2007 to investigate his level of cognitive and emotional functioning, to make recommendations towards semi-independent living and to suggest potential accommodations for taking the General Educational Development (GED) exam. Neuropsychological testing showed the patients abilities are overall low-average. Premorbid abilities were estimated as average. Academic achievement was variable. He demonstrated low-average reading skills, borderline impaired math skills and impaired written expression. Language was generally normal but his fluency was slowed. Motor skills were impaired due to tremors, slowness, and likely sensory loss. Fine motor dexterity was impaired bilaterally.
Medical History:
Psychiatric History
Family psychiatric history: It is positive for alcoholism. Both father and mother have been abusing alcohol. Patient’s paternal aunt has a history of depression
Social and Developmental History: The patient is the youngest of three siblings. He reached developmental milestones without delay. The patient repeated the fourth grade and had difficulties in school which required special classes and tutoring, prior to his brain injury. The patient was in Learning Disability (LD) classes all along. The patient’s parents were married for 13 yrs before getting separated. The patient was 5 years old at that time. There is no history of any physical or sexual abuse as a child. The patient completed his sophomore year of high school. He tried to return to high school without success after his brain injury. The patient has not previously held a job over an extended period. The patient is not married and has no children. He currently lives with his girlfriend. There have been two incidents of legal problems following the accident, one involving an obscene phone call which led to his arrest and another involving a violent outburst (throwing furniture) while living at a residential facility.
On-going issues: The patient is successful with his basic activities of daily living (ADLs). He is dependent for instrumental activities of daily living (IADLs), such as finances. The patient has many symptoms, including cognitive problems, such as executive dysfunction (disorganization, poor planning, lack of initiative), memory loss, word finding difficulties and poor concentration. The patient has been consistently struggling with irritability, depression, alcohol dependence, mood dysregulation, poor impulse control with frequent anger outbursts and loss of confidence. The patient continues to struggle with paranoia. Physical symptoms with which the patient has been dealing include tremors, vision and coordination problems.
Literature Review Results
What follows now is a review of literature where the results of the patient’s workup are presented in the form of tables. The results are presented in the form of ‘yes/no/unknown’ or ‘content’ responses. A brief explanation of results is also provided in this section.
Figure 1

From the review of the records it is not clear if the patient received any initial resuscitative measures when the ambulance arrived at the scene. The patient did not have any history of previous head injury.
Figure 2

The patient did not undergo aggressive resuscitative measures in the ER as the patient did not have any significant blood loss. The use of steroids in severe TBI is not a standard practice29 and records do not provide evidence for or against the use of steroids. Monitoring of jugular venous oxygen saturation, use of hyperventilation and the different methods to help identify brain ischemia are also the usually used practices in the management of TBI24 and there is no proof whether these methods were or were not employed.
Figure 3

The patient had clear cut indications for admission to the hospital. The other reasons for admission did not seem to apply to the patient.
Figure 4

Patient’s vitals were monitored constantly. Neurological checks were done every four hours and included monitoring pupillary size and reactivity. Frequent monitoring of the GCS was not found on the review of hospitalization records.
Figure 5

There are no records from the Cognitive Rehabilitation Services and the Center for Cognitive Services where the patient was admitted following discharge from the initial hospitalization and again several years later. Unfortunately no records could be obtained.
Figure 6
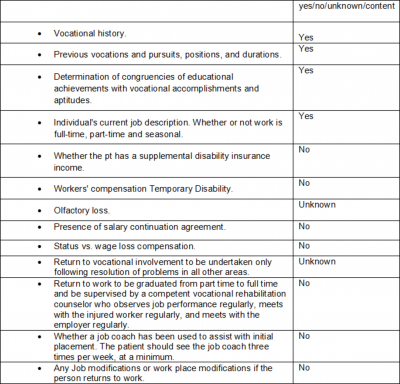
The patient has never undergone any kind of vocational rehabilitation including any kind of assistance from a job coach.
Figure 7

Psychological evaluation and education for different things, as indicated in Table 7, has not been done. Documentation for any such prior efforts is not available.
Figure 8
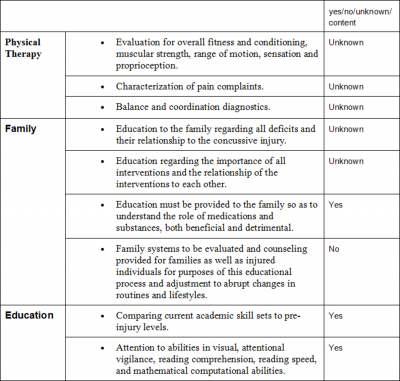
There was lack of overall information regarding physical therapy. Family education seemed to have been a part of initial hospitalization. Family education regarding the deficits and the relation of the deficits to traumatic brain injury was not in the available record. The patient and the family did get education about the role and the effect of psychiatric medications.
Figure 9

Recommendations were made based on the results of the neuropsychological testing which included encouragement for successful semi-independent living, incorporating structure into patient’s everyday activities and weekly therapy sessions to develop coping skills and interpersonal skills. Recommendation regarding taking GED included extended test taking times (twice the usual), use of calculator and tutoring for written expression. Job recommendations included use of an occupational therapist, part-time entry-level position, reduced social interaction and working closely with a job coach. From a clinical standpoint, expectations that the patient could follow the recommendations appear excessive.
Figure 10

Table 10 indicates the different psychiatric conditions that can occur following TBI and whether the patient was evaluated for these conditions or not. Previous records are not available to indicate any evaluation for frontal and temporal lobe syndromes but since the patient’s care in Loyola, this evaluation has not been conducted. No evaluation for Somatization, Hypochondriasis, Malingering or Secondary gains seems to have been done and records for such evaluations are not available. The most likely explanation of why evaluation for secondary gains or malingering has not been done is that the patient is already on disability and has not demonstrated such behaviors.
Figure 11

Figure 12
Figure 13

After multiple attempts at obtaining information from each of these places over a course of 5 months, after prior authorization from the patient, none was received. The only records that could be obtained were from the mother regarding the first hospitalization, but even those records are not complete.
Discussion
An attempt is made to condense the results of literature search and focus on the psychiatric manifestations of TBI. Examples are presented with the objective of demonstrating how learning about a case should proceed from textbook to review articles to current literature and this is suggested as a model way of learning and teaching.
The current Diagnostic and Statistical Manual –IV-TR (DSM-IV-TR) has a limited classification system with respect to the definition of mild, moderate, or severe TBI. Post Concussional Disorder is mentioned in Cognitive Disorder Not Otherwise Specified and Appendix B of the DSM-IV-TR provides criteria sets and axes for future studies. TBI can be subdivided into mild, moderate, and severe to help predict outcome. A commonly used severity classification system in TBI uses the Glasgow Coma Scale (GCS), the duration of Post-Traumatic Amnesia (PTA) and the Loss of Consciousness (LOC) as determinants of severity41. Prognosis becomes worse with the severity of injury, but mild TBI is more poorly defined and prognosis is not as clear with it41.
Figure 14

The utility of different scales varies in assessing cognition and behavior during the phases of recovery from TBI. The scales that can be used for this purpose include GCS9j, 9k, 18, 19, Galveston Orientation and Amnesia Test (GOAT)9k, 9n, 36, Rancho Los Amigos Scale9k, 9m, Neurobehavioral Rating Scale (NRS)9k, 37 and Neurobehavioral Cognitive Status Examination (NCSE)9k, 38.
In the case presented, GCS had been used at the time of the initial evaluation in the ER. There is no mention of its use in the records thereafter. The GCS is commonly used for the initial assessment of severity9j. It is a clinical prognostic indicator9j and contributes to early assessment of the severity of brain injury. Assessment on arrival at the emergency room is recommended9j. The GCS remains one of the most consistently utilized measures of brain injury severity9j. The GCS seems to have been appropriately used in the case since it was used at the time of initial evaluation but not thereafter and, perhaps, should have been. The Galveston Orientation and Amnesia Test (GOAT) can be used to follow the course of improvement in the PTA following emergence from coma and can be used to establish the end of this period9n, 36. The length of PTA may correlate with the outcome of psychiatric and behavioral sequelae9e, 19. The GOAT score correlates with the severity of injury and is helpful in predicting the long-term outcome9k. Review of the patient’s records did not reveal the use of GOAT. Nothing is known about the duration of PTA in the index case. It could have helped determine the end point of coma. The duration of PTA is an indicator of the severity of injury and is a clinically useful predictor of outcome following TBI9e, 55 and could have helped predict psychiatric and behavioral sequelae.
The Rancho Los Amigos Scale is a useful tool in tracking cognitive and behavioral recovery9k. Since the patient was diagnosed as having suffered a severe TBI; he was expected to have a number of neurobehavioral changes. Recovery from severe TBI is marked by a number of stages and these stages can be documented and followed using the Rancho Los Amigos Cognitive Scale. Patient’s neurobehavioral recovery progressed from level II to level + VI/-VII on this scale. The intervening stages of recovery are not documented in the patient’s record and this may demonstrate inconsistent use of this scale. The Neurobehavioral Rating Scale (NRS) is a useful tool in assessing neurobehavioral functioning in TBI patients9k, 37. It offers a way of quantifying change over time9k, 37. The Neurobehavioral Cognitive Status Examination (NCSE) assesses levels of consciousness, attention and orientation, language and visuoconstructional skills, memory, calculations and abstract reasoning and is an extremely useful tool for rapid cognitive screening9k, 38. Neither NBSE nor NBS scales were used.
Two of the widely used scales in assessing outcome of acute brain injury are the Glasgow Outcome Scale (GOS)9i, 12-17 and the Disability Rating Scale (DRS)12, 13, 15, 54. “One criticism of scales of disability and handicap such as the GOS is that they fail to capture the subjective perspective of the person with head injury.” 14 The GOS is considered to be a crude indicator of medical complications or residual effects at the time of discharge from the primary treatment center9i. Psychiatric illness is significantly more common among the patients who show unfavorable outcome according to the Glasgow Outcome Scale 1 year after traumatic brain injury1. The DRS more sensitively reflects improvement during in hospital rehabilitation than the GOS, 71% to 33%, respectively15. The DRS is a sensitive, functional, reliable, and quantitative means of monitoring patients with TBI during the course of their recovery15. Neither of these scales has been used. Use of GOS would have enabled to determine residual effects at the time of the initial discharge. The DRS can help in a similar manner. This could have provided with some idea about the psychiatric illnesses that the patient may develop at a later stage in life and therefore be of prognostic value. The lengthy review of evaluative scales to establish and monitor the patient’s clinical status is done to illustrate the large number of potentially available instruments that are available that have immediate and prognostic value.
The patient has been diagnosed and treated for depression ever since his discharge from his first hospitalization. The patient has had problems with concentration, insomnia, irritability, loss of confidence and loss of libido. He has also had depressed mood, psychomotor retardation, lack of motivation and emotional blunting as well as lability. The symptom overlap between depression and apathy makes it difficult to tease the two apart. He could be having both apathy and depression at the same time although the mechanisms involved may be different. The consistent feature in diagnosing depression is depressed mood. In diagnosing the patient’s depression the DSM –IV criteria have been used. The patient has also engaged in alcoholism which may have further complicated the picture. The differential diagnosis of post-TBI depression can include adjustment disorder with depressed mood, apathy, emotional lability, substance induced mood disorder and post traumatic stress disorder (PTSD) 9b. The frequency of Depressive Disorders following TBI varies from 6-77 %9b. This is due to the fact that many of the studies that report prevalence of depression following TBI have relied on cut off points on rating scales like the MMPI or relatives’ reports rather than structured interviews and diagnostic criteria (e.g. DSM-IV)9b. Patients with TBI are at great risk for developing depressive symptoms49. Depression following TBI can be associated with executive dysfunction, negative affect, and prominent anxiety symptoms50. Symptoms of major depression such as sleep, appetite, lack of interest or libido changes may occur in patients with TBI as a consequence of brain injury or as a consequence of acute medical illness with hospitalization9b. Therefore, these symptoms that are used to diagnose depression may occur independent of the associated mood symptoms and consequently depression can be overdiagnosed9b. The reverse can also be possible and patients may deny the presence of depressed mood as a part of a denial syndrome which could lead to under diagnosis of depression9b. Some of the features that are associated with depression during the acute phase after TBI such as anxiety, initial insomnia, diurnal mood variation and decreased appetite and weight loss may be clinical manifestations of a biologically determined depressive syndrome9b. On the other hand, terminal insomnia, loss of libido and diminished ability to think and concentrate, which are significantly associated with depression only after 6 months post-TBI may be symptoms that emerge only after the acute effects of TBI have subsided and some recovery has taken place9b.
TBI patients may present with apathy syndrome which is frequently associated with psychomotor retardation and emotional blunting9b, 10. Although apathy may frequently be associated with frontal lobe damage, there are no studies that have systematically studied the relationship between apathy and the type, extent and location of TBI9b, 10. The symptoms that are specific to depression change over time in post-TBI depression and this suggests that the nature of post-TBI depression changes over time9b. Biological factors may also play a role in the pathogenesis of post-TBI depression. Premorbid psychological and social impairments increase the risk of developing significant depressive disorders following TBI9b. Head injury has been found to produce neurotransmitter and neurohormonal changes consistently. Changes in the level of serotonin, dopamine, epinephrine and nor-epinephrine are postulated9b. No double-blind, placebo-controlled studies are available that have studied the efficacy of different pharmacological treatments of post -TBI depression9b. Selection of the anti-depressant is guided by the side effect profile. Anticholinergic activity, seizure lowering threshold potential and sedation are some of the side effects that may be considered in the choice of antidepressant medication9b, 41.
In the examples cited above, literature review has proceeded from textbook to review articles to current literature. Using a textbook provides baseline knowledge about the subject. Textbooks are detail oriented and cover all the major aspects of the subject up to the date of publication. However, new editions of textbooks may not be published in the coming four or five years. Since there is a delay in the latest research and literature reaching a textbook, it does not always provide recent advances and trends in the area. There may be possible gaps that are left in the literature if textbooks are used as the only source of review and there is a certain possibility that the area of interest has progressed further since the textbook was last published. Some of these gaps can be filled by researching review articles and the current literature. Use of review articles and current literature tend to consolidate what is already known and well established on the subject and also provide with the latest knowledge on current trends, fields of interest and latest research. Thus, the gaps are filled and knowledge can proceed on a continuum from textbook to review articles to current literature. Moving in such a manner in a literature search on any subject can provide an ideal foundation for learning purposes and this method has been used in exploring for information about the case presented in this report. The section on depression is used to illustrate this pattern of learning. From the textbook, facts about post-TBI depression including its prevalence are learned. The reason for a wide range in prevalence is described. The over-reliance of the studies on rating scales that use cut off points for diagnosing depression is striking. There have not been many prevalence studies of post-TBI depression. From the review article it is observed that one of the challenges in using the DSM –IV criteria for diagnosing post-TBI depression is that the effect of TBI on somatic and motivational symptoms may occur independently of effects on mood. For example, sleep disturbance, fatigue, apathy and concentration difficulties are common signs and symptoms in TBI survivors with and without mood disorders40. The addition of depressed mood to this list will result in meeting criteria for major depressive disorder. As a result, there is a chance that the prevalence of post –TBI depression may be overestimated if unmodified DSM criteria are used40. Finally, review of recent literature indicates that major depression is a frequent complication of TBI that hinders a patient’s recovery50. Major depression is associated with negative affect, executive dysfunction and anxiety symptoms50. The neuropathological changes produced by TBI may lead to deactivation of lateral and dorsal prefrontal cortices and increased activation of ventral limbic and paralimbic structures including the amygdale and this may play a significant role in the complex pathophysiology of post-TBI deression50.
One of the major difficulties that was encountered during the course of reviewing patient records was obtaining outside records. Multiple attempts did not seem to help in obtaining records. Several reminders in the form of faxes and letters which included patient authorization to release medical records were sent to the different places listed in Table 13 without success. Many conclusions can be drawn to explain why medical records could not be obtained. The human effort involved in collecting the records and then sending them to the concerned parties is enormous. Very few individuals will be willing to undertake that task on a voluntary basis unless it is a part of their job. It would involve locating the records, making copies of the records and then either mailing them or faxing them. It would be hard for anyone to take time out of their busy schedule to accomplish all these tasks when there is no expectation of either a reward or reprisal. Presence or absence of Electronic Medical Records (EMR) does not seem to influence obtaining records from outside sources. The expectation with EMR is that medical records are easy to locate and can be faxed without difficulty. Again, the human effort involved in the entire process seems to be a big factor and lack thereof seems to have resulted in the failure to obtain the records.
Conclusions
Comparing the actual evaluation, treatment and management of a patient, suffering a particular condition, with the medical literature can provide an excellent opportunity for learning. The literature review should progress from the textbook to review articles to current literature. Clinical practices do not always follow the medical literature recommendations or guidelines and a complete and thorough evaluation as recommended by the review of the literature is not always achieved. Obtaining information from different location and sites is unpredictable and time consuming. Information obtained from the patient and family may not always be reliable and may contradict the information in records, therefore, it is hard to draw conclusions regarding different treatments received by the patient during the course of the disease.
Appendix I: Glasgow Outcome Scale (GOS)
1. Dead
2. Vegetative state
3. Severe Disability
Able to follow commands/ unable to live independently
4. Moderate Disability
Able to live independently; unable to return to work or school
5. Good Recovery
Able to return to work or school
Appendix II: Disability Rating Scale (DRS)
Figure 15

Figure 16

Disability Categories
Appendix III: Glasgow Coma Scale (GCS)
Figure 17

Appendix IV: Rancho Los Amigos Scale
I. No Response: Unresponsive to any stimuli.
II. Generalized Response: Limited, inconsistent and nonpurposefully responses-often to pain only.
III. Localized Response: Purposeful responses; may follow simple commands; may focus on presented object
IV. Confused-Agitated: Heightened state of activity; confusion and disorientation; aggressive behavior; unable to do self care; unaware of present events; agitation appears related to internal confusion
V. Confused-Inappropriate, Non-Agitated: Nonagitated; appears alert; responds to commands; distractible; does not concentrate on task; agitated responses to external stimuli; verbally inappropriate; does not learn new information
VI. Confused-Appropriate: Goal-directed behavior, needs cuing; can relearn old skills such as activities of daily living; serious memory problems; some awareness of self and others
VII. Automatic-Appropriate: Appears appropriately oriented; frequently robotlike in daily routine; minimal or absent confusion; shallow recall; increased awareness of self and interaction in environment; lacks insight into condition; decreased judgment and problem solving; lacks realistic planning for future
VIII. Purposeful-Appropriate: Alert and oriented, recalls and integrates past events; learns new activities and can continue without supervision; independent in home and living skills; capable of driving; defects in stress tolerance, judgment and abstract reasoning persists; may function at reduced level in society