Femoral Nerve Block: Provided By Nysora - New York School Of Regional Anesthesia
A Hadzic, J Vloka
Citation
A Hadzic, J Vloka. Femoral Nerve Block: Provided By Nysora - New York School Of Regional Anesthesia. The Internet Journal of Anesthesiology. 2002 Volume 6 Number 2.
Abstract
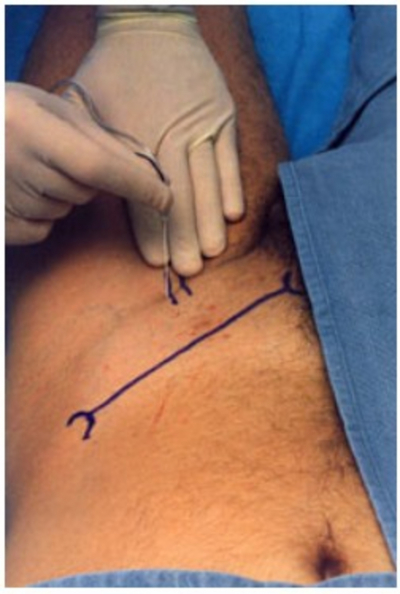
Demonstration of a femoral nerve block
Based on:
Vloka JD, Hadzic A, Reiss W,Drobnik L, April EW, Sanborn K, Thys, DM. Femoral Nerve Block: Needle Insertion at the Inguinal Crease Results in more Consistent Nerve Localization. Reg Anesth Pain Med 1998; 23(3):53.
Figure 6

Introduction
A commonly suggested approaches to femoral nerve block involve insertion of the block needle 1-2 cm lateral to the femoral artery just below the inguinal ligament, regardless of the technique (nerve stimulator, paresthesia, double click, arterial pulsation, infiltration, etc.).
Figure 2

Attempt to femoral nerve block frequently requires multiple attempts at localization of the femoral nerve, and yields inconsistent success rate. Performing the block at the level of the inguinal skin crease however, has given us more consistent results in our practice. Below is a description of this new technique.
Figure 3

Description of the Technique
A 22G, 50 mm short bevel insulated needle attached to nerve stimulator (0.6 mA) is inserted adjacent to the lateral border of the
Figure 4
If a quadericeps muscle twitch is not obtained, the needle is withdrawn and
Figure 5

Considerations
The optimal site of needle insertion when performing the FNB, is the inguinal crease level. Advantages of performing the block at the inguinal skin crease level over performing the block at inguinal ligament level are:
-
More superficial position of the femoral artery and nerve,
-
Greater width of the femoral nerve,
-
More consistent femoral nerve-artery relationship.
{image:6}
Copyright © 1998-2002 NYSORA.
With permission of the authors and NYSORA. In collaboration with The Internet Journal of Anesthesiology. Find more information about NYSORA by clicking here!