A Comparative Clinical Study Of Tramadol V/S Pentazocine For Sedation And Analgesia As Premedication (A Study Of 60 Cases)
V TRIVEDI
Citation
V TRIVEDI. A Comparative Clinical Study Of Tramadol V/S Pentazocine For Sedation And Analgesia As Premedication (A Study Of 60 Cases). The Internet Journal of Anesthesiology. 2009 Volume 26 Number 1.
Abstract
This randomized clinical study was conducted in 60 ASA I-II patients undergoing spinal anaesthesia for lower limb orthopedic surgery and lower abdominal surgery with Tramadol and Pentazocine as premedication. All patients were monitored for haemodynamic stability,pulse,B.P.,RR,SPO2,ECG and sedation score before premedication, after premedication, 15min, 30min, 45min intraoperatively as well as postopertively up to 24hrs. Group I (n=30 ) received injection Tramadol (1mg/kg) and injection Glycopyrrolate(4mcg/kg) intramuscularly and group II (n=30 ) received injection Pentazocine (1mg/kg) and injection glycopyrrolate(4mcg/kg) intramuscularly 45min prior to surgery. In group I haemodynamic stability was maintained better than in group II p value (0.05) significant. For postoperative analgesia in group I and II VAS score was 2 and 3 respectively at 6hrs. Intraoperative sedationscore in group I and II was 2(awake and calm) and 3(deep sleep and arousable) and postoperatively it was 1(wide awake) and 2 in group I and II respectively. No major side effects were observed in any patient of both groups. So Tramadol has a better haemodynamic stability and postoperative analgesia as compared to Pentazocine but sedation is achieved better with Pentazocine than Tramadol.
Introduction
Preanaesthetic medication is a term applied to use of drug prior to administration of anaesthetic drug so as to provide sedation, anxiolysis, analgesia, amnesia, antiemesis, counteract adverse effects of anaesthetic drug like salivation, vagal stimulation and vomiting.
Opioids used as premedication to allay anxiety and provide analgesia is popular technique. The word opioid is derived from opos,the Greek word for juice, the drug being derived from juice of opium poppy, Papaver Somniferum1 Opioids exert their analgesic effect through mu, kappa, delta receptors. Supraspinal analgesia of opioid is through inhibition of ascending transmission of nociceptive information from spinal cord dorsal horn. Local spinal mechanism through inhibition of substance P. Opioids also has peripheral mechanisms to provide analgesia.
Many synthetic opioids share side effects of natural opioids. Tramadol synthetic 4-phenyl-piperidine analog of codine with a dual mechanism of action. It stimulate mu receptor ,lesser extent delta and kappa, it also activates spinal inhibition of pain by decreasing re-uptake of norepinephrine and serotonin. It is one fifth to one tenth as potent as Morphine. It has less effect on respiratory and gastrointestinal system.
Pentazocine provide analgesia primarily related to kappa receptor stimulation. It is one half to one fourth as potent as Morphine. It has a high incidence of nausea, vomiting, respiratory depression, dysphoric effects. It can produce undesirable cardiovascular and psychomimetic effects.
Methods
The study was conducted for 60 ASA Grade I-II patients age between 21-50 yrs for routine surgery under spinal anaesthesia like lower limb orthopedic surgery and lower abdominal surgery. After taking routine informed consent all patients were divided equally into 2 groups.
Group I (n= 30) received injection Tramadol (1mg/kg) and injection Glycopyrrolate (4mcg/kg) intramuscularly 45min prior to surgery. Group II (n= 30) received injection Pentazocine (1mg/kg) and injection Glycopyrrolate (4mcg/kg) intramuscularly 45min prior to surgery. Preoperatively routine investigations of blood, urine, ECG Chest X-ray were within normal limit and major cardiovascular and metabolic disorder were excluded. all patient were monitored preoperatively for haemodynamic stability pulse, B.P.(non invasive) ECG, SPO2 for 15min, 30min, and 45min after premedication and during induction and intraoperatively at interval of 15min as well as postoperatively up to 24hrs. All Patients were monitored for sedation score and postoperative analgesia.
Sedation score as described by Chernik et al
Score 1- wide awake
Score 2- awake and calm
Score 3- deep sleep but arousable
Score 4- deep sleep but not arousable
All patients were educated before premedication for VAS score where
No pain
10- worst pain which is not bearable
Postoperative analgesia was administered when VAS score more than 3 with injection Diclofenac 75mg intramuscularly.
In addition complications like nausea, vomiting hypotension, hypertension, tachycardia, bradycardia, respiratory depression were also monitored after premedication, during anaesthesia and also postoperatively.
We used paired ‘t’ test for statistical analysis. Formula
t = x
-----
sn
where t= t value
x = mean of difference
s = standard deviation of difference
n = sample size
p value considered significant when < 0.05
Results
Figure 1

This table shows no difference in age, weight,and sex distribution in both the groups.
Figure 2

As shown in table II and charts 1,2 , in all patients after premedication 45min mean pulse rate in Group I was 85.1±7.27 (mean ± SD) per minute and 88.4±7.17 (mean± SD) per minute in Group II and difference in both the Group was significant (p <0.05) and also postoperatively at 6hr mean pulse rate in Group I was 85.1±7.27 (mean ±SD) per minute and in Group II 88.4±7.17 (mean ±SD) per minute and difference in both Groups was significant.
During intraoperatively and postoperatively 3hr,12hr and at 24hr difference in both the groups was not significant (p>0.05).
Mean arterial pressure after premedication 45min, after induction of anaesthesia immediate, 15min, 45min, 60min, 120min and postoperatively at immediate, 3hr, 6hr all differences in both Groups was significant (p<0.05) before premedication, after induction of anaesthesia at 30min, 90min, and postoperatively at 12hrs and 24hrs difference is not significant (p>0.05)
Figure 3

Figure 4
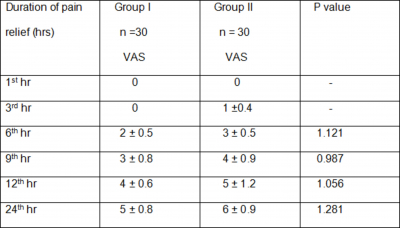
VAS score in Group I is less than that of Group II. So postoperative analgesia was better in Group I than in Group II.
Figure 5

In Group I two patients (6.67%) had nausea , one patient (3.33%) complained of vomiting. In Group II three patients (10%) complained of nausea and vomiting and one patient (3.33%) had hypertension and tachycardia.
Figure 6

Figure 7

Figure 8

Figure 9

Figure 10

Discussion
Premedication term was first used by Makenon and Clement in 1920 in an article by American editor anaesthetist frank Hoffer Memcham. The same term was used by Sigton in 1929 and Hewer in 1932 in his first edition of ‘Recent advances in anaesthesia’1-4
Opioids have been administered for hundreds of years to allay anxiety and to reduce pain associated with surgery. The present study was carried out to compare the effect of both drugs Tramadol and Pentazocine for postoperative analgesia, degree of sedation, cardiovascular changes, respiratory changes and of adverse effects in patient given premedication.
Katz WA5 studied the efficacy of Tramadol as analgesic in patients undergoing orthopedic procedures of upper and lower limb. 25 patients were taken and were given Tramadol before surgery as premedication, duration of analgesia was 6 to 8.5hrs without any effect on cardiovascular and respiratory depression.
D. A. Laffey and N. H. Kay6 in 1984 studied premedication with Tramadol a comparison with Morphine. They used Tramadol 50mg and Morphine 10mg as premedication intramuscularly in two group of patients during general anaesthesia and regional anaesthesia. they observed Tramadol provides effective premedication as Morphine producing fewer side effects like drowsiness with requirement of post operative analgesia earlier than Morphine. Pain relief with Tramadol was obtained for 8 to 10hrs and with Morphine for 14 to 16hrs but with side effects like dry mouth, dizziness and painful injection site and respiratory depression.
Cardiovascular changes were observed with Pentazocine due to sympathomimetic effects and rise in plasma Epinephrine and Norepinephrine by Pentazocine as documented by Sigman et al and Tammisto et al 7,8. study was done 50 patients of lower abdominal and orthopedic surgeries with regional anaesthesia. They concluded that rise in mean pulse rate and mean arterial pressure was 20 to 30% from that of before premedication.
Tramadol had rapid onset and longer duration of action and greater analgesic effect than Pentazocine.this was observed in study done by William C. North and D. R. Tielens9. Tramadol causes better pain relief without respiratory depression10.
Less nausea and vomiting with less requirement of analgesic with Tramadol was observed in study done by Yung Fung Sung et al11 in 30 patients undergoing endoscopic procedures.
Conclusion
In present study Tramadol (1mg/kg) and Pentazocine (1mg/kg) intramuscularly is optimum dosage for premedication, cardiovascular changes was more with Pentazocine group. Pain relief was better Tramadol group and of longer duration than Pentazocine and sedation was more and of longer duration with Pentazocine group. Tramadol having short duration of onset and longer action with no or low incidence of side effects like nausea and vomiting an effective , safe premedication drug .