Laparoscopic diagnosis and management of an inflamed epiploic appendage with torsion and necrosis
B Papaziogas, I Koutelidakis, P Tsiaousis, C Christoforakis, K Atmatzidis
Keywords
acute abdomen, epiploic appendage, inflammation, torsion
Citation
B Papaziogas, I Koutelidakis, P Tsiaousis, C Christoforakis, K Atmatzidis. Laparoscopic diagnosis and management of an inflamed epiploic appendage with torsion and necrosis. The Internet Journal of Surgery. 2008 Volume 20 Number 2.
Abstract
Acute epiploic appendagitis, caused by torsion, inflammation and necrosis of an appendix epiploica, is a rare clinical entity that can be easily misdiagnosed as acute appendicitis or diverticulitis. We report a case of a 23-year-old male, who presented to the emergency department complaining of an intense and persistent abdominal pain, localized to the left lower quadrant, accompanied by nausea. The suspicion of epiploic appendagitis was established by the findings of a contrast-study computed tomography of the abdomen. A diagnostic laparotomy was subsequently undertaken due to clinical deterioration of the abdominal pain despite antibiotic coverage. A necrotic epiploic appendage of the descending colon was revealed, which was removed laparoscopically. Laparoscopic exploration, diagnosis and secure management in acute abdominal conditions is highly recommended in the surgical literature and its value was proven once again in the herein presented case.
Introduction
Epiploic appendages, referred also as “appendices epiploicae” are small peritoneal fat pouches, between 0.5 and 5cm long, which are attached to the external surface of the colon by vascular stalks (one or two arterioles and a venule), originating in two rows, anterior and posterior, parallel to the taenia coli 123 . Their first anatomical description was done by Vesalius (in 1543) and Virchow (in 1853), who noticed that their detachment might be a source of “free intraperitoneal bodies”.
Torsion of an epiploic appendage occurs rarely, but it can result in ischemia and inflammation, presenting as an acute clinical condition such as diverticulitis, appendicitis, cholecystitis, pancreatitis, urinary tract infections or other cases of acute abdomen 14 . The areas of the colon, that are most commonly affected, are, in decreasing order of frequency, the sigmoid colon, the ceacum, the descending colon and the ascending colon 567 . Furthermore, spontaneous venous thrombosis of an appendageal draining vein is another cause of primary epiploic appendagitis 38 .
On clinical examination, the pain is usually located in the left or in the right lower abdominal quadrant 39 . Due to the lack of pathognomonic clinical features the diagnosis is often difficult, delayed or completely missed 3 . A CT scan of the abdomen provides significant help, leading to the rare diagnosis of epiploic appendagitis, avoiding unnecessary surgery in some patients 3510 .
Case report
A 23-year-old male, otherwise healthy, with no significant previous medical or surgical history presented to the medical department complaining of acute left lower quadrant pain of 12-hour duration. The patient described his pain as dull, constant and exacerbating by acute movements. He reported anorexia and nausea but denied any episodes of vomiting. He remained afebrile.
Physical examination revealed a young man in mild distress with normal vital signs. Moderate tenderness including guarding and rebound was elicited in the left lower quadrant. Bowel sounds were lowered but audible. The findings from the remainder of the physical examination were normal.
Significant lab exams included a mild leukocytosis (WBC= 10500/mm 3 ), while the rest were within normal range.
A contrast computed tomography study of the abdomen and pelvis was obtained, which revealed a thin-walled, oval-shaped, 22 x 8mm lobule of fat, in contact with the descending colon and the parietal peritoneum wall and surrounded by minimal haziness observed in the adjacent adipose tissue (Fig. 1). This finding was located in the most inferior aspect of the descending colon.
Figure 1
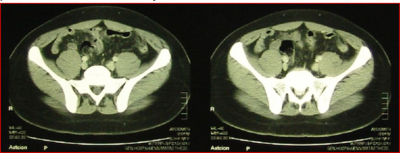
The patient was admitted to the hospital for observation and antibiotics were commenced. Despite the conservative treatment, the patient’s clinical status deteriorated within hours. The decision was taken to proceed with a diagnostic laparoscopy, whereupon an inflamed, twisted and necrotic epiploic appendage of the sigmoid colon was discovered. Untwisting of the inflamed appendage, ligation with metallic clips, excision and finally retrieval of the specimen in a zipper-type sterile plastic bag formed the sequence of the intraoperative actions (Video). The postoperative course was of three days duration and was unremarkable.
Discussion
Epiploic appendages are small pouches of peritoneum, each of which is supplied by vascular stalks, which protrude from the external serosal surface of the colon into the peritoneum 21112 . They occur in the rectosigmoid junction (57%), ileoceacal region (26%), ascending colon (9%), transverse colon (6%) and descending colon (2%) 56 . The pedunculated shape, the free range of movement and the tortuous nature of their blood supply makes epiploic appendages vulnerable to torsion or ischemic change 111 .
The term “epiploic appendagitis” was introduced by Lynn et al. in 1956 to describe the rare inflammatory process that results from a disturbance in the vasculature such as torsion or venous thrombosis of the epiploic appendage involved. The sigmoid colon is more commonly affected than the ceacum and men are more frequently affected than women 211 .
The exact physiological functions of epiploic appendages are not yet clarified. It has been proposed that their role involves a soft support cushioning of the colon, a role in immune response (much like that of the lesser omentum) and colonic absorption. A twisting, kinking or stretching of epiploic appendages along their long axis with impairment of their vascular supply results in subsequent venous thrombosis and necrosis (sometimes hemorrhagic). Although less likely, primary thrombosis is also possible.
On clinical exam, patients usually describe a localized, strong, non-migratory sharp pain, which commenced after a specific movement of their body, during postprandial exercise for example 29 . Abdominal tenderness is present. There is usually a lack of fever, vomiting or leukocytic response but a slight increase of CRP value 81112 .
Ultrasound sometimes shows an oval-shaped, non-compressible hyperechoic mass with a subtle hypoechoic rim, directly under the site of maximum tenderness 13 . Moreover, normal epiploic appendages are not seen on a CT scan, unless they are surrounded by intraperitoneal fluid or inflammation 410 . In 1986, Danielson et al. were the first to report a case of epiploic appendagitis diagnosed by CT scan 410 . Pathognomonic CT findings include a 2-4cm oval-shaped, fat-density lesion, with a hyperdense ring surrounded by inflammatory changes. Thickening of the parietal peritoneum wall may sometimes be also observed 48101314 .
There is a variety of complications described that often follow on epiploic appendagitis, such as the formation of adhesions 12 (as the result of surrounding inflammation), the appearance of focal abscesses (simulating a neoplastic lesion), intussusception, bowel obstruction 15 and peritonitis. Rarely, “peritoneal loose bodies” (infracted and not definitely inflamed epiploic appendages) cause intestinal obstruction or urine retention, depending on their size and localization 451013 .
The indicated therapy of epiploic appendagitis is still a matter of controversy. It is widely accepted that this clinical entity is self-limiting, with patients recovering in less than 10 days, when given anti-inflammatory and antibiotic medication 23 . Most of the surgical literature supports the benign course of this disease and favors a conservative therapy. However, it is also observed that there has been a tendency of recurrence in conservatively treated patients and therefore some surgeons believe that surgical therapy might finally prevent recurrence, inflammation induced adhesions and other less common complications 51114 . Furthermore, laparoscopic interventions are highly appealing to both patients and surgeons in the form of exploration via a laparoscopic approach with simple ligation and excision of the inflamed appendage 111 . The benefit of short hospitalization, quick mobilization and avoidance of unnecessary irradiation exposure by the use of multiple follow-up CT scans is clearly accepted. On the other hand, there can occur complications such as excessive bleeding, infection or an unexpected reaction to the anesthetics as well as specific complications of laparoscopy like accidental damage of internal organs or abdominal bruising, which have to be discussed with the patient 314 .