Hypoglossal Schwannoma In The Submandibular Region
K Misawa, Y Asai, S Iwasaki, H Mineta
Keywords
hypoglossal nerve, mri, schwannoma, submandibular region
Citation
K Misawa, Y Asai, S Iwasaki, H Mineta. Hypoglossal Schwannoma In The Submandibular Region. The Internet Journal of Otorhinolaryngology. 2005 Volume 5 Number 2.
Abstract
Hypoglossal schwannomas usually develop in the intracranial portion of the brain. The incidences of hypoglossal schwannomas of the submandibular region are extremely rare. We reported a case of schwannoma arising from the extracranial hypoglossal nerve in the submandibular region.
Introduction
Schwannomas (neuromas, neurilemmomas) are benign tumors originating from Schwann cells or nerve fiber sheath cells. They are a solitary, encapsulated tumor usually attached to, or surrounded by a nerve, and are not associated with von Recklinghausen's disease. (1) Schwannomas of the hypoglossal nerve usually develop in the intracranial portion or both in the intracranial and the extracranial components forming a dumb-bell shape. (2) Hypoglossal schwannomas of the peripheral segment are extremely rare, and several cases have been reported in English literature. (3) We present herein a case of hypoglossal nerve schwannoma originating from the submandibular space.
Case Report
A 58-year-old male presented a mass in the left submandibular region 5 years ago. During a physical examination, a soft, painless, well-defined, and tender mass formation was discovered, without evidence of atrophy or paralysis on the left half of the tongue. There were no skin nodules or lesions, and no cafe'au lait spots.
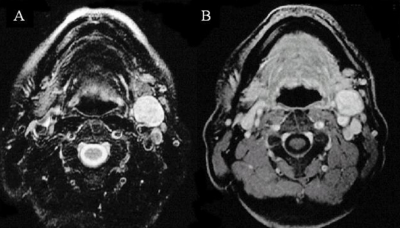
Magnetic resonance imaging (MRI) showed that a 25×20×18mm well-circumscribed mass was present in the dorsal part of the submandiblar glands. On a T2-weighted image, the mass showed a hyperintense tumor containing focal ill-defined hypointense areas. The tumor appeared slightly higher in intensity than that of the muscle, showing marked nonhomogenous attenuation on the postgadolinium T1-weighted image. (Figure 1A, B)
Figure 1
During an operation, a well-encapsulated mass was found deep within the left submandibular gland. The hypoglossal nerve was identified, entering in the proximal pole of the tumor and running distally out of the tumor. Because it was impossible to dissect the hypoglossal nerve from the tumor, we sacrificed the nerve and removed it along with the tumor.
Grossly, they are yellow or yellowish-gray in appearance. (Figure 2A) Histological examination revealed that the tumor was schwannoma and consisted mostly of Antoni A type with focal Antoni B type tissues. (Figure 2B)
Figure 2

After the operation, the patient suffered from slight dysphagia resulting from the mild atrophy and the right-side tongue deviation. However, the hypoglossal nerve paralysis does not affect his daily life and the patient is in good health. The patient has remained free of disease and without symptoms for more than 5 years from his original diagnosis.
Discussion
Schwannomas originate from Schwann cells located at the sheaths of peripheral, cranial or autonomic nerves. (1) Many authors have reported that schwannoma occurs regardless of age or sex, and grows slowly and painlessly. (1,2,3,4) In the head and neck, schwannomas usually arise from the sensory divisions of cranial nerves, most commonly the vestibular nerve and the vagal nerve. (4) Hypoglossal schwannoma is very rare because hypoglossal nerve consists of only a motor component. (4) The purely motor hypoglossal nerve emerges from the medulla oblongata between the pyramid and the olive, passes extracranially through the hypoglossal canal, and describes a wide ventral curve between the internal jugular vein and the internal carotid artery to the floor of the mouth. The parent tumor was located in the submandibular space surrounded by the submandibular gland, a space which is an unusual site for schwannoma. (5) Other differential diagnoses for tumors in the submandibular space include benign pleomorphic adenoma, infectious disease and nodal metastases. (3)
Macroscopically, they appear as single, well-circumscribed, encapsulated masses. Microscopically, two types of tissue co-exist, distributed randomly in schwannoma. Schwannoma contains both Antoni A type tissue with interwoven bundles of long, bipolar, spindle cells, and Antoni B type tissue with its loose texture. Nuclear palisading in some areas was also typical. (2,5)
MRI resulted in an excellent demonstration of peripheral neurogenic tumors with good delimitation to attached structures using gadolinium contrast enhancement. Schwannomas are isointense to muscle on T1-weighted images and show more hyperintense than muscle on T2-weighed images, and show intense contrast enhancement. The high T2 signal represents myxomatous degenerative of the schwannoma, as seen peripheral component of this tumor, whereas the central low T2 signal correspond in hypovascular fibrous and collagenous portion. (4,6)
Pleomorphic adenomas are the most common of all benign tumors of submandibular gland origin. They occur as slowly growing, solitary, well-demarcated masses with a capsule of variable thickness and completeness. (2) Pleomorphic adenomas may be indistinguishable from schwannomas on MRI imaging feature alone. (2,6)
We reported a case of hypoglossal schwannomas in submandibular space. Although schwannoma in submandibular space is very rare, when a well circumscribed mass is observed, as with the present case, schwannoma should be taken into consideration on making a differential diagnosis. We believe that total excision of the tumor
Acknowledgements
We are grateful to Mr. Andrew B. Cole for his helpful advice.
Correspondence to
Kiyoshi Misawa, MD, Otolaryngology-Head and Neck Surgery, Hamamatsu University School of Medicine. 1-20-1 Handayama, Hamamatsu-City, 431-3192, Japan Tel: +81-53-435-2252 Fax: +81-53-435-2253 E-mail: kiyoshim@sis.seirei.or.jp