Self, Social, and Family Perceptions in Relation to Loneliness Controlling for Depression among Individuals with Schizophrenia
D Tharayil
Keywords
depression, family relations, loneliness, schizophrenia, self-perception, social perception
Citation
D Tharayil. Self, Social, and Family Perceptions in Relation to Loneliness Controlling for Depression among Individuals with Schizophrenia. The Internet Journal of Mental Health. 2006 Volume 4 Number 1.
Abstract
Introduction
Loneliness is a significant problem for people without a formal psychiatric diagnosis, as well as for people with clinically diagnosed psychopathology (1, 2) and for some it is a chronic condition (3). In psychology, loneliness has generally been defined as an unpleasant, aversive, and distressing experience or feeling
The size and quality of one's social network can determine the degree of loneliness among people. Weiss (6) contended that when one's relational interactions are deficient and one's social network provisions are less than expected, one becomes easily vulnerable to experience loneliness. An individual at this point can experience interpersonal isolation and feelings of abandonment resulting in a sense of utter aloneness and loneliness. Freeney (7) added evidence to Weiss in linking loneliness to a person's attachment to significant figures in life. Absence or reduced quality of connectedness to important attachment figures like parents can result in a decreased sense of belonging to others and social network disturbances which eventually can contribute to the rise of loneliness.
As commented by Gerstein and colleagues (8) one psychiatric disorder that has consistently been discussed in terms of its association with loneliness is schizophrenia. According to a Government report, 3.2 million Filipinos suffer from mental disorders (9). A statistical report taken during 2000-2003 at the National Center for Mental Health, Philippines (NCMH) indicates that schizophrenia is the highest of the ten leading causes for psychiatric consultation and hospitalization. It is unfortunate to know that loneliness of psychiatric patients is given very little attention in psychological research. As perceptions or thoughts of lonely people are important in evaluating their experience of loneliness and in interventions because lonely people are usually identified with negative self and social perceptions (10), this study is relevant in this context.
Giving emphasis to the cognitive processes like perceptions of the lonely, certain researchers (11, 12, 13) proposed that loneliness occurs when an individual perceives a discrepancy between the desired and the achieved pattern of social relations. The cognitive bias model (14) suggests that some people tend to hold pervasive negative perceptions of themselves and of the world in general, predisposing them to evaluate themselves as neurotic, worthless, and lonely. Rokach (15) identified negative self-perceptions of lonely people that include feeling unimportant, unattractive, or simply unable to offer anything significant to others. Reviews by Christensen and Kashy (10) show that self-perceptions of social skills deficits, self-perceptions of low social support, and self-perceptions of unattractiveness are linked to loneliness. Anderson and Riger (16) identified that lonely persons have cynical and pessimistic attitudes, selective attention to negative information about them, believe that their life is uncontrollable, and that they are unworthy of others' affection. The result is social withdrawal, failing to make close relationships, reduced social networks, and thereby loneliness. The problem becomes aggravated when the individual suffering from loneliness is afflicted with schizophrenia because a few of the negative symptoms of schizophrenia are emotional and social withdrawal and apathy (17) which can lead to a social network crisis (18). Also, the quality/capacity of the social network can have a major influence on both mental and physical health.
According to some studies, social perceptions of lonely people in various aspects appear to be more negatively biased. Wittenberg and Reis (19) observed that lonelier participants are more deficient in relationship formation and maintenance skills, and hold more negative perceptions of others. Lonely individuals recognize their social deficits, and expect others to recognize them as well and hence reject them. They believe that others would be less interested in and accepting of them. These persons then express less interest in and acceptance of others, resulting in the experience of loneliness (20). Also, lonely individuals may possess a general pessimistic attitude or cognitive representation that people cannot be trusted or that others will reject them due to their perceived social incompetence (21, 22, 23).
Certain studies examined lonely people's perceptions of family. Although the studies on the perceptions of family among lonely individuals with schizophrenia are not available, the following information would show how those with schizophrenia might view their family regarding family functioning. Communication deviance (CD), problems in expressed emotion (EE), and affective style (AS) have been empirically identified as strong characteristics of families with a member affected by mental illness, especially schizophrenia (24). Communication deviance refers to a family's disturbed style of communicating with one another, and is believed to contribute to negative perceptions regarding family experiences among persons affected by schizophrenia. The incidence of schizophrenia and related disorders within the family was found to be highest in those families classified as high in communication deviance, although no causal relationship was established (25). Reviews done by Goldenberg and Goldenberg (26) report high levels of expressed emotion among the family members of those with schizophrenia. These families tend to express high levels of criticism, guilt inducing statements, emotional over-involvement, or signs of hostility (extreme expression of negative feelings) directed towards the affected individual. Affective style involves the patient and his or her family discussing a topic that has been a source of conflict in the past.
Cutting and Docherty (27) identified factors on the perception of those with schizophrenia and their parents' attitudes and its association with relapse. Those who perceived their parents as low in care (i.e., indifferent and rejecting) and high in protection (over-involvement) had a severe course of illness if they had frequent contact with such parents. This situation could emotionally isolate the individual with schizophrenia from the family network and thereby result in loneliness.
It is evident from psychiatric information that depression and schizophrenia sometimes coexist in the same patient. Post-psychotic depression is a phenomenon occurring after the acute phase of schizophrenic illness (28). Research among those without mental illness shows a relationship between depression and loneliness (29). Also, depression is strongly associated with emotional loneliness, whereas anxiety is related to social isolation. Since depression and loneliness can coexist in lonely individuals affected by schizophrenia, this study takes a precautionary measure to statistically control the possible confounding effect of depression in the analysis of perception variables in relation to loneliness (30).
The purpose of this study is to explore and identify if self, social and family perceptions would be significantly related to loneliness after statistically controlling for depression among persons with schizophrenia. Number of years with schizophrenia and the age of the participants were also included in this analysis.
Method
Participants
Participants were 35 Filipino adult men with schizophrenia (27-44 years old; M = 36.7 years). This included 15 participants (43%) from the National Center for Mental Health and 20 (57%) from the Plainview Home Care Psychiatric Center situated in Metro Manila, Philippines. Although there were a large number participants affected by schizophrenia in these centers, the choice of participants was based on the following criteria: participants must be diagnosed with schizophrenia based on DSM-IV criteria at the time of admission; age should not exceed 45 years, schizophrenia should not be substance induced, participants were not given antidepressants, the medical chart should indicate that the participants were ready to be discharged and going home, and that they were in remission of overt psychotic symptoms (i.e. even the residual symptoms should not interfere their normal communication with people and the researcher). The researcher even made sure the participants were free from common annoying side effects like rigidity or tremor due to antipsychotic medications. Their usual medications were antipsychotic drugs like chlorpromazine, haloperidol, and fluphenazine
Female participants were not included in this study due to various reasons. Most of the women in these centers did not meet the criteria because a large number of women were suffering from major depression rather than from schizophrenia.
Regarding the social network and support experiences, 27 (77%) participants were not involved in intimate relationships at the time of data collection and 8 participants (23%) had troubled marital relationship and fear of abandonment although living with their spouses and children. The participants had to discontinue their jobs due to their illness and all of them depended on their respective families for their care. It was assumed that these social network deficiencies and need for dependency could contribute to their loneliness, negative perceptions of self, social relationships, and family.
Research Instruments
An appropriate attempt was undertaken to create face validity and to ensure reliability of all instruments used in this study for collecting data in the Philippine context. A number of psychologists, psychiatrists, and a psychiatric nurse checked the language and the content to ensure that the participants would be able to answer the items without difficulty according to the Philippine cultural context and the educational status of the participants. Their comments and suggestions were noted and followed. After following these suggestions, pilot testing of the instruments was done. Participants of the pilot study positively confirmed that they were able to respond to the items easily. The participants of the pilot test were not included in the actual test administration.
Procedures
The ethical committee of research in social sciences, which is the Dissertation Committee of the College of Social Sciences and Philosophy at the University of the Philippines, thoroughly reviewed the proposal for research on psychiatric patients to ensure that the ethical policies of the Declaration of Helsinki were strictly followed. The researcher obtained permission from each psychiatric center to collect data for research after agreeing to follow all requirements of the centers regarding research policies.
The researcher invited the qualified participants individually according to their availability and explained the nature of research. Informed consent was obtained to ensure their voluntary participation and confidentiality. All precautions were taken to prevent any moral or emotional damage to the participants that might incur during or after the data collection, especially due to self-disclosure. The participants were given freedom to withdraw from the study at any moment if they found it threatening. Participants were cooperative. Ample time was allotted to the participants in data gathering process. Individual administration of the instruments to a participant took approximately 45 minutes.
The scores of the revised UCLA Loneliness Scale were used as the criterion measure for loneliness. The scores of the standardized self-report inventories to measure Self, Social, and Family Perceptions, and Depression were used as the predictor variables. The scoring of all instruments was done manually according to the directives given for each instrument. The scores for the number of years in illness and age were derived from the demographic data. SPSS version 11.5 was used for encoding data and statistical analysis. Bivariate correlations, partial correlations, simple linear regression analysis, and hierarchical multiple regression analysis were conducted to answer the hypotheses.
Results
Descriptive Characteristics of Variables
Table 1 presented the demographic characteristics of the participants. These demographic data are not considered in the analysis except for the number of years with schizophrenia and the age of the participants.
Figure 1

The dependent variable of loneliness had a mean score of 40.5 (
Correlation and Predictive Relationship between Self-Perceptions and Loneliness
This study hypothesized that negative self-perceptions are positively and significantly correlated with loneliness of individuals with schizophrenia. In support of this hypothesis, data that appear in Table 2 shows that there is a significant positive relationship (
Further, it was hypothesized that negative self-perceptions would independently and significantly predict loneliness. The coefficient of determination indicates that negative self-perceptions account for 24% of the changes in the degree of loneliness.
Regression coefficients of the model are displayed in the summary output in Table 3. As the
Correlation and Predictive Relationship between Social Perceptions and Loneliness
It was also hypothesized that social perceptions would independently and significantly predict loneliness. The coefficient of determination indicates that negative social perceptions only account for 9% of the changes in the degree of loneliness. Table 3 shows the regression results (
Figure 2

Correlation and Predictive Relationship between Family Perceptions and Loneliness
The hypothesis that the negative family perceptions would be positively and significantly correlated with loneliness among persons with schizophrenia was only partially confirmed. Data in Table 2 show that there exists a moderate positive relationship between negative family perceptions among participants and their loneliness (
Spearman's rho correlation coefficient of the relationship between perceptions of family and loneliness indicated that there is a moderately significant positive relationship between negative perceptions of family and loneliness
Correlation and Predictive Relationship between Depression and Loneliness
The relationship between depression and loneliness (see Table 2) is positive and significant (
Predictive Relationship of the Number of Years in Illness and Age with Loneliness
Additional findings on the predictive relationship of the number of years with schizophrenia (
Figure 3

Partial Correlation Coefficients Controlling for Depression
Variables of number of years with illness and age were not included in the partial correlation analysis because of their non-significant relationship with loneliness. Table 4 shows the partial correlation coefficients of self-perceptions, social perceptions, and family perceptions by controlling for depression. It shows that the coefficient values of the variables of perceptions declined when the portion of variation that is shared by depression was controlled. The coefficient value
Figure 4

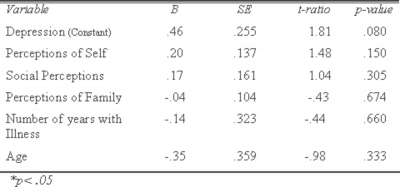
Hierarchical Multiple Regression Analysis Holding Depression as a Covariate
It was hypothesized that self, social, and family perceptions, the number of years with illness and the age of the participants would significantly predict loneliness when depression is held as a covariate. This was tested by the following analysis using Hierarchical
In Table 5 for coefficients, the unique predictive relationship of depression with the outcome variable of loneliness appears to be insignificant at .05 (
Figure 5
Discussion
Negative Self-Perceptions Related to Loneliness
The findings show that there is a significant positive relationship between negative self-perceptions and loneliness and that these negative self-perceptions independently and significantly predict loneliness. The possible contributors to this finding could be the negative beliefs of self that might have emerged from the attitudes and behaviors of family members and those outside family towards the participants even in childhood years in various forms and aggravated when they were affected by schizophrenia. Based on the relevant literature in this study, it is assumed that these negative self-perceptions can have a long history in its development and incorporation into the personality of the participants. Narratives of experiences in the developmental stages of these participants have shown that they had negative childhood and family related experiences (40). It is very likely that problems in self-perception might have developed from these early experiences and could have predisposed the person to experience loneliness. Narrative information from the same participants (40) can corroborate this finding. Almost 83% of the participants had very poor self-belief and 73% were very dissatisfied with themselves. Self-deprecatory thoughts like no courage to face people, they were not likable or lovable, and they were stupid, dull, incompetent and inefficient, worthless and useless, morally bad and ugly were prevalent among them. Many participants were thinking about themselves in a very pathological manner as if their “personal self” had lost its identity. Definitely these negative thoughts have clinical implications. However, establishing the causality of negative self-beliefs due to the onset of schizophrenia is beyond the scope of this study. Nevertheless, these observations call for significant attention for clinical interventions in dealing with loneliness.
The significant link between negative self-perceptions and loneliness observed in this study is in accordance with many previous findings. The association between severe loneliness and poor self-perceptions or self-esteem is one of the consistent findings in studies on loneliness based on reviews. A number of studies confirm that there is a link between loneliness and negative self-perceptions of social skills and unattractiveness (10, 12), negative perceptions of worthlessness and being unloved (41), and poor self-esteem (14).
Wood (42) tries to explain the relationship of loneliness to low self-esteem from several different causal processes. Low self-esteem or poor self-perception may be both a cause and a consequence of loneliness. It is said that low self-esteem can foster loneliness and loneliness can impair self-esteem. Low self-esteem is often rooted in an interrelated set of self-defeating cognitions and behaviors that impair social competence which predispose a person for loneliness. Another causal process is that severe and prolonged loneliness can decrease a person's self-regard. The social network mediation model (14) explains that people with low self-esteem have difficulty establishing and maintaining social relationships and therefore are lonely. The cognitive bias model (14) suggests that self-reports of loneliness are more a function of intrapersonal negative cognitive processes. The presence of schizophrenia among the participants of this study may delimit this kind of explanation since the illness itself could take a heavy toll in the area of perceptions of the affected person.
Anderson and Riger (16) present a cyclic process of negative self-beliefs begetting poor self-esteem that begets social withdrawal which deprives people of close relationships resulting in loneliness that produces still low self-esteem and thus forming a vicious cycle as represented in Figure 1.
Figure 6

Peplau and colleagues (12) also suggest that self-blaming attributional style might predispose a person to experience loneliness or the combined effect of low self-esteem and social incompetence that interferes with initiating or maintaining satisfying social relations can contribute to the emergence of loneliness.
These explanations may clarify why persons affected by schizophrenia felt lonely as their negative self-perceptions are linked to loneliness.
Predominance and Mediating Influence of Negative Self-Perceptions in This Study
Partial correlation results (see Table 4) by controlling for depression showed significant relationships only between negative self-perceptions and loneliness suggesting that even without the confounding effect of depression on loneliness, negative self-beliefs maintained its significant relationship with loneliness. This would lead to a conclusion that the negative mindset is a strong contributor to the increase of loneliness. This is consistent with previously cited findings, which show that low self-esteem contributed nearly double of what negative social perceptions and depression did (14, 16, 43). In the current study, when depression was controlled, negative self-perceptions correlated with loneliness much higher than negative social and family perceptions (see Figure 2).
Figure 7

This inference is relatively confirmed from bivariate correlation results (see Table 2) that negative self-perceptions are more significantly related to loneliness than they are with depression. This would strengthen the assumption that persons with loneliness could be influenced more by negative self-perceptions than by depression if these variables are viewed from a triangular relationship. Additional tests showed that negative self-perceptions independently accounted for variances in depression only 20.5% while they could independently explain 24% of variances in loneliness. This suggests that in the triangular relationships among negative self-perceptions, loneliness, and depression, negative self-perceptions would predict loneliness better than they would in depression. A recent study (44) added further evidence to this observation. In a model that included loneliness as well as depression as dependent variables, self-esteem was significantly related to both. This model indicated that problems in self-esteem accounted for 56% of the variance in loneliness and 41% of the variance in depressive symptoms.
The inference that negative self-perceptions contribute more to loneliness than to depression is all the more justifiable because researchers (45) suggest that there are other ways to understand depression than looking at it through loneliness. If explained further, all lonely people would also be labeled as depressed, not the other way around. It means that it is more probable for a lonely person to complain about feeling depressed than for a depressed person to complain about feeling lonely. This suggests that both loneliness and depression could be better clarified through a very likely common factor of negative self-perceptions.
Additional strengthening information in favor of the impact of negative self-perceptions on all variables of this study after controlling for depression is that when depression is controlled, the only variable that is still significantly correlated with loneliness, negative social and family perceptions, is negative self-perceptions. Further, it is noticeable from intercorrelations (see Table 2) that the only variable that is significantly correlated with all other variables of interest including depression is the negative self-perceptions suggesting that this variable has most likely the highest mediating function and predominance among other variables of interest in this study. This might strengthen the suggestion that the negative self-perceptions could be either a predisposing or a maintaining factor for loneliness. One significant factor noticed is that negative self-perceptions share variances significantly with both loneliness and depression, though not equally, signifying that a set of self-derogatory beliefs is a probable common factor in these negative emotional states.
According to the observations of Hansson (46) subjective quality of life in people with a severe mental illness is not so much dependent on external life conditions, but on reducing the symptoms of depression, anxiety, and strengthening aspects of the social network. Personality-related factors such as self-esteem are also influential.
In mental health promotion among people suffering from schizophrenia, it is worthwhile to focus on assessing their self-perceptions to prevent them from plunging into unhealthy thoughts and feelings of uselessness and worthless which might lead them to social withdrawal resulting in loneliness.
Negative Social Perceptions Related to Loneliness
It was observed in this study that negative social perceptions positively and significantly correlated with loneliness. In some cases it is likely that participants might have experienced negative responses from others contrary to their expectations. Certain studies that report on the social perceptions among lonely people generated information only on what others would be thinking about the participants like such as less open, less socially skilled, less likable, attractive, and friendly indicating a consistent tendency in lonely people to think that others evaluated them more negatively (10). People prefer information that matches their self-perceptions even if those beliefs are negative predisposing them to distortions in their social perceptions.
Moreover, a number of personality characteristics have been linked to biased social perceptions. Reviews done by Levin & Stokes (14) indicate that loneliness is repeatedly linked to cynical and rejecting attitude toward other people. Some evidence shows that lonely people as compared to non-lonely people hold more negative social perceptions (19). It is assumed according to Markovsky (47) that there is a close relationship between the perceptions that are formed and the subsequent actions taken on their behalf. Most probably the participants of this study might have detached themselves from people because of their negative social perceptions eventually producing loneliness.
Negative social perceptions in relation to loneliness may be explained in a reasonable way again by what Jones (20) had noticed. Pessimistic attitudes reduce the likelihood of continued interpersonal contact from which a satisfying relationship might emerge. It has been identified that loneliness emerges from the failure to exercise or maximize interpersonal opportunities. There is also evidence to suggest that lonely individuals may possess a cognitive representation that people cannot be trusted or others would reject them due to their perceived social incompetence (21). This is corroborated by other studies, which propose that lonely persons have a general pessimistic attitude toward social situations (22). The cognitive bias model (14) could also be helpful to explain the significant relationship. Negative beliefs on others are interpersonal cognitive processes that predispose persons to have distrust towards others, which inhibit them from establishing relationships. The residual cognitive deficits affecting perception, attention, and memory have many consequences like harming social functioning, employment, and quality of life. Negative symptoms due to schizophrenia are also deficits in feeling pleasure, speech production, emotional expressiveness, and social interaction. These contribute to the social incompetence and asociality. This situation in fact could reduce the size of their social network (48, 49).
Schizophrenia could create a social network crisis. The social network is significantly weaker in persons affected by schizophrenia as compared to those with physical disease (18). However, it is very difficult to establish if social network problems are directly caused by the onset of schizophrenia. It may in fact exist prior to the illness (50) and it may be due to existing characteristics in the personality, or social and family issues. However, the existence of paranoid thinking in relationships of people affected by schizophrenia cannot be overlooked. It is difficult for people who perceive others with suspicion to build trustworthy relationships and this would eventually affect the quality and quantity of social interactions and responses to social support. Their asocial tendencies could be connected to the perceptions they keep regarding people. Nevertheless, comparative studies have shown that patients in community care settings with good social network access have a better subjective quality of life than patients in hospital settings. In fact narrative report (40) showed that most of the participants of this study positively perceived social support from their families. This may be because in the Philippines persons with schizophrenia are cared well by their own family members. In any case, a social network therapy program for clients with schizophrenia and loneliness could be very helpful to increase the quality of their existing relationship with people, rather than searching for a large number of people and contacts where they might experience rejection and isolation.
Apart from the aforementioned reasons associated with negative self and social perceptions, social network issues are associated with frequent and long-term hospitalizations and being away from family and neighborhood (51), and negative symptoms (52, 53). A significantly worse social network compared to a normal sample both in quantitative and qualitative aspects of the network is a great possibility for persons with schizophrenia. Relatives and friends turn out to be the patient's main source of supportive contacts according to Bengtsson-Tops & Hansson (53).
Negative Family Perceptions Related to Loneliness
Spearman's rho correlation yielded a significant positive relationship between negative family perceptions and loneliness. Nonetheless, the predictive relationship between these variables did not yield a significant result. Only 6.6% of the variance in loneliness was explained by the changes in the negative perceptions of family. Certain extraneous factors might have contributed to this trivial result. Participants' social desirability characteristic could play a role in the nature of data. This factor might have inhibited participants from giving truthful information of the reality and so it is likely that the participants wanted to present a favorable family image by evaluating most of the items positively. It is understandable from the Philippine context of family values and ties (54) that most people may consider disrespectful for the family, should members of the family divulge their family problems to a stranger or to others who are not connected to them. Objective measures usually face social desirability problems in item responses (55).
Nevertheless, quality of satisfaction with one's family relationships predicted the degree of loneliness better than frequency of contact with family or distance from home. Reviews regarding this topic consistently lead to a conclusion that the higher the satisfaction with parental relationships, the lower the degree of loneliness, and the degree of warmth, closeness, and love reflect how one learns to relate with others (41, 56). Restrictive parents employ rules which are to be strictly followed and disobedience would incur punishment. Previous research has confirmed that rejection and restrictiveness, cold, disapproving, and punitive attitudes continue to create negative influence in later years and are related to loneliness (57, 58). Shaver and Rubenstein (59) suggest that there is vulnerability for adult loneliness, for which a causal path can be traced back to experiences in infancy and childhood. It has been reported that children of hostile parents seem to be deprived of emotional softness demonstrating a variety of neurotic symptoms like social withdrawal, which increases the likelihood of loneliness (60). In another study, significant relationships were found between the relatives' poor empathic attitude and the patients' occupational functioning and social relations suggesting that empathy in the relative is an independent predictor of social functioning in people with schizophrenia (61). In support of this, the current study demonstrates that negative family perceptions are significantly related to negative social perceptions (see Table 2 & 4). If therapists would like to deal with the loneliness of persons with schizophrenia, they should definitely assist them to improve their social functioning by educating family members to have empathy and understanding towards the affected family member.
Depression Related to Loneliness
The finding on the relationship between loneliness and depression shows that there is a highly significant positive relationship between these two variables among the participants affected by schizophrenia. This suggests that when the degree of loneliness increases, there is a corresponding rise in the intensity of depression and vice versa. Although exploring depression in relation to loneliness was not the major objective of the study, it was included in the study to isolate depression in the analysis of other variables. Even if depression and negative self-perceptions are significantly related to loneliness with equal significance, the correlation coefficient of an independent relationship between depression and loneliness is slightly greater than that of negative perceptions of self and loneliness. It means that depression independently is the best predictor of loneliness in this study.
The finding of this study concerning depression in relation to loneliness is consistent with many previous results (29, 30) regardless of the clinical status of the participants. In other words, depression is associated with loneliness in non-clinical populations as well as in people affected by schizophrenia. This suggests that depression is an unhealthy companion of loneliness. This does not mean that those with schizophrenia suffer a higher degree of depression than other clinical and non-clinical populations with loneliness. In fact, Neeleman and Power (62) observed a lower degree of depression among those with schizophrenia as compared to people with clinical depression and suicidal tendencies. Although a significant relationship between depression and loneliness is a fact even in non-clinical samples (63), in their study depression did not significantly account for the variances in loneliness, contrary to the finding of the current study. Linear regression analyses showed that depression is the best predictor in this study and depression independently accounted for 25% of the variances in loneliness, while negative perceptions of self was the second best predictor which significantly accounted for 24% of the changes in loneliness.
The current study infers from the above observations that coexistence of loneliness and depression in those with schizophrenia is a possibility only if their self-perceptions are more pessimistic. However, depression has been attributed to schizophrenia itself. It has been noticed that there is an acute phase of illness and 50% of those with schizophrenia suffer a marked depression at the beginning of hospitalization (28). But little is known about the depression of those with schizophrenia who are in the state of remission of overt psychotic features. If this study makes use of the explanation of Horowtiz, French, and Anderson (45) regarding the presence of loneliness as a strong indicator of depression and not vice versa, it is reasonable to think that the presence of loneliness may be an antecedent of depression among the participants of this study, not that schizophrenia acts as an antecedent of depression. However, this has to be validated by further studies.
The presence of depression among participants of this study could be due to multiple factors like self-blaming attributional style (12) and low self-esteem (64). A recent study identified that depression and poor self-esteem were correlated among individuals with schizophrenia (65) and thus strengthening the influence of negative self-perceptions in the origin and continuance of loneliness in the life of individuals affected by schizophrenia.
Conclusion
Various findings of predominance and mediating influence of negative self-perceptions bring evidence that coexistence of loneliness and depression is a possibility only if self-perceptions of persons affected by schizophrenia are more pessimistic and self-derogatory. Even when the confounding effect of depression on loneliness is controlled, negative self-perceptions could still be a significant predisposing and maintaining factor of loneliness. As negative self-perceptions could adversely affect the quality and quantity of social network contacts, it is highly suggested to initially deal with the issue of negative self-perceptions in order to bring out effective social and family relationships and thereby reduce loneliness and the risks associated with it. Efforts to improve the quality of life of people with schizophrenia should also include a careful monitoring of depression and particular attention to the satisfaction of unmet needs within the person's domains of self, social connections, and family. The small sample may limit generalization and future research should examine the experience of women too.
Acknowledgements
This research was supported with a Faculty Research Grant of the University of the Philippines, as the author is teaching in the same University as Assistant Professor of Psychology, Clarkfiled, Pampanga. The author gratefully acknowledges the contributions of Dr. Juliet C. Mallari, and the administrators and participants from National Center for Mental Health and Plainview Homecare Center, Mandaluyong City, Philippines, Dr. Violeta V. Bautista and other reviewers in the completion of this work.
Correspondence to
Davis Porinchu Tharayil, PhD Assistant Professor Department of Psychology University of the Philippines Clark Airbase, Angeles City-2009 Philippines e-mail: davisptin@yahoo.co.in