Protocols for Nutrition Support of Neuro Intensive Care Unit Patients: A Guide for Residents
C Ghanbari
Keywords
ards, cardiac, cardio-pulmonary support, critical care, critically ill, education, emergency medicine, head injury, hemodynamics, intensive care, intensive care medicine, intensivecare unit, medicine, multiorgan failure, neuro, nutrition, patient care, pediatric, respiratory failure, surgical i, ventilation
Citation
C Ghanbari. Protocols for Nutrition Support of Neuro Intensive Care Unit Patients: A Guide for Residents. The Internet Journal of Emergency and Intensive Care Medicine. 1998 Volume 3 Number 1.
Abstract
Patients with neurological disorders often require non-oral nutrition support beca
use of intubation, altered mental status or dysphagia, irrespective of surgical in
tervention. To maximize patient outcome, nutrition support must be initiated withi
n a 48- to 72-hour window immediately post-injury or surgical insult. In an attemp
t to provide nutrition support in an uniform manner without unnecessary delays, a
multidisciplinary team of physicians, nurses, speech pathologists and the unit die
titian developed a set of nutrition support protocols for use in the neuro intensi
ve care unit at our institution. Although new residents receive a handbook with ex
tensive references on nutrition support, a brief orientation on the protocols and
a one hour nutrition support lecture, a need was identified for a concise, pocket-
sized reference outlining the fundamentals of nutrition support and the unit's nut
rition protocols step-by-step. Towards this end, the unit dietitian developed a si
x-page nutrition support reference in outline form that is reproduced here. Althou
gh the material is geared towards the neurosurgical patient, it provides nutrition
support basics appropriate for nearly any intensive care patient population. The
material covers selection of an appropriate feeding route, assessment of nutrition
al status and nutrient requirements, calculation of parenteral and enteral feeding
regimens, monitoring of nutrition support patients, and weaning patients off of n
utrition support onto oral diets.
Glossary of Medical Terms and Abbreviations
-
A (vitamin): retinol
-
ARDS: adult respiratory distress syndrome
-
BEE: basal energy expenditure
-
BM: bowel movement
-
B12 (vitamin): cobalamin
-
C. Diff: Clostridium difficile
-
CHF: congestive heart failure
-
CHI: closed head injury
-
C V V H:continous veno-venous hemofiltration
-
CAVHD: continuous arterio-venous hemodialysis
-
d: day
-
dl: deciliter
-
DHT: Dobhoff tube (brand name for nasoenteral feeding tube)
-
E (vitamin): tocopherol
-
FIO2: forced inspiratory oxygen
-
FSBG: fingerstick blood glucose
-
GI: gastrointestinal
-
H2 blocker: histamine-2 blocker
-
I & O: intake and output
-
IBW: Ideal Body Weight
-
K (vitamin): phylloquinone, menaquinone, and/or menadione
-
K+: potassium
-
Kcal: kilocalorie
-
kg: kilogram
-
KUB: abdominal x-ray
-
mg: milligram
-
ml: milliliter
-
mMol: millimol
-
mEq: milliequivalent
-
MSOF: multi system organ failure
-
n/a: not available
-
Na+: sodium
-
NJT: nasojejunal tube
-
PEEP: positive end-expiratory pressure
-
PEG: percutaneous endoscopic gastrostomy
-
PEJ: percutaneous endoscopic jejunostomy
-
p.o.: per os (by mouth)
-
PPN: peripheral parenteral nutrition
-
REE: resting energy expenditure
-
RQ: respiratory quotient
-
SIADH: syndrome of inappropriate anti-diuretic hormone
-
TG: triglycerides
-
TPN: total parenteral nutrition
-
TSBA: total body surface
-
ug: microgram
-
VE : minute ventilation
-
VO2: volume of oxygen consumed
-
VCO2: volume of carbon dioxide produced
INTRODUCTION
Neurologically impaired patients often require non-oral nutrition support because of intubation, altered mental status or dysphagia. Common diagnoses of patients admitted to a neuro intensive care unit (NICU) include traumatic head injury, stroke, brain tumor, spinal cord injury, degenerative disease (multiple sclerosis, amyotrophic lateral sclerosis, Alzheimer’s, Parkinson’s) or a mobility disorder (myasthenia gravis, Guillain-Barre syndrome). All of these conditions have the potential to promote visceral protein depletion and wasting of skeletal musculature through dysmobility, inadequate oral intake or hypercatabolism secondary to the disease process. Even non-surgical patients may be in a hypermetabolic, hypercatabolic state due to the nature of their disease and the invasive interventions required to support them during treatment and recovery. 1
Early nutrition support through the enteral route has been shown to blunt catabolism, reduce complications and reduce length of stay in a number of patient populations, including both surgical and non-surgical neuro patients. 2,3 However, nutrition support must be initiated within the 48- to 72-hour period immediately following injury or surgical insult to achieve these benefits. 2 Clinicians are often hesitant to feed critically ill neuro patients too soon. However, studies indicate patients with severe neurological deficits and clinically silent abdomens can tolerate low-rate jejunal feedings within 36 hours of injury 4 with a gradual increase in feeding rate to meet initial caloric goals within two to four days. 4,5 If jejunal feedings are initiated prior to induction of pentobarbital infusion, even patients in pentobarbital coma can be fed enterally. 6
In an attempt to provide nutrition support in an uniform manner without unnecessary delays, a multidisciplinary team of physicians, nurses, speech pathologists and the unit dietitian developed a set of nutrition support protocols for use in the neuro intensive care unit at our institution. The team also developed pre-printed orders to be used in conjunction with the protocols. The primary responsibility for initiating and monitoring nutrition support lies with a team of NICU residents in collaboration with the attending physician, nursing staff and the unit dietitian.
New residents receive a brief orientation on the protocols and an ICU handbook with extensive references on nutrition support on their first day of rotation. Later in the month, the residents attend a one-hour lecture on nutrition support. Nevertheless, a lack of nutrition support knowledge was identified among NICU residents that the orientation, handbook and lecture did not adequately address. As a result, nutrition support was often delayed or inappropriate. A need was identified for a concise, pocket-sized reference outlining the fundamentals of nutrition support as per the unit protocols in a step-by-step fashion to assist the residents in writing nutrition support orders.
Towards this end, the unit dietitian developed a six-page nutrition support reference in outline form that is reproduced here. Although the material is geared towards the NICU patient, the basic information it provides is appropriate for nearly any intensive care patient population. The material covers selection of an appropriate feeding route, assessment of nutritional status and nutrient requirements, calculation of parenteral and enteral feeding regimens, monitoring of nutrition support patients, and weaning patients off of nutrition support onto oral diets. The reference is not designed to be all-inclusive, adding to its ease of use by residents in a busy intensive care unit where many nutrition support regimens must be initiated, adjusted and monitored daily.
Protocols
Figure 1

II. Assess the patient’s nutritional status and nutrient requirements.8
Figure 2

Figure 3

Male: BEE = 66.47 + (13.75 x weight in kg) + (5.0 x height in cm) - (6.76 x age in years)
Female: BEE = 655.1 + (9.56 x weight in kg) + (1.85 x height in cm) - (4.68 x age in years)
III. Begin feeding through chosen access route as soon as patient is hemodynamically stable and oxygenating well. Benefits of early nutrition support as described in the literature occur when feedings are initiated within 48 to 72 hours following injury or surgical insult.2 Feeding a hemodynamically unstable patient may lead to undesirable complications, most notably bowel infarction in enterally fed patients.
Figure 4

Figure 5

V. Protocol, enterally-fed patients 7,13
NOTE: Bowel sounds are an unreliable indicator of small bowel function. Patients with altered GI function may be fed with elemental solutions via the small bowel in most instances. Continuous small bowel feedings are associated with a lower incidence of feeding-induced GI dysfunction and a higher incidence of achieving and maintaining feeding goals in the ICU setting than with gastric or bolus feedings.14
Figure 6

Figure 7
VI. Protocol for parenterally fed patients, central access10
Figure 8

VII. Protocol for parenterally fed patients, peripheral access7,10
Figure 9

If patient meets all 4 criteria, start peripheral nutrition to provide > 75% calorie/protein needs
If patient does not meet all 4 criteria, start support via central line or reconsider enteral feedings
Figure 10

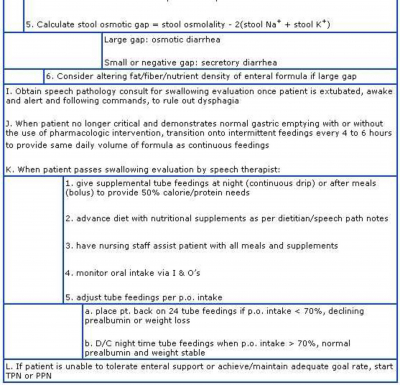
VIII. Monitor the patient and adjust nutrition support as indicated8,10,11,12,13
Figure 11

IX. Parenteral Electrolyte Requirements
Figure 12

Potassium and sodium are available as phosphorus or chloride, or as acetate, a bicarbonate precursor. Calcium is available as gluconate or chloride. Magnesium is available as sulfate.
X. Parenteral Electrolyte and Vitamin Requirements in Acute or Chronic Renal Failure19
Figure 13
