Intramuscular Angioma of the Frontalis Muscle
M Chen, D Sarma
Keywords
frontalis muscle angioma, hemangioma, intramuscular angioma
Citation
M Chen, D Sarma. Intramuscular Angioma of the Frontalis Muscle. The Internet Journal of Dermatology. 2006 Volume 5 Number 2.
Abstract
A case of intramuscular angioma in the frontalis muscle of the forehead is reported. The etiology, pathology and treatment of this rare tumor are briefly reviewed.
Introduction
Intramuscular angioma, a member of deeply located hemangiomas, represents less than 1% of all hemangiomas[1], and is mostly seen in young adults of both sexes. Only 15% of the intramuscular angiomas are located at the head and neck region[2]. We are reporting such a case occurring in the frontalis muscle of the forehead.
Case Report
A 41-year-old white male noticed a small, soft, nontender mass on his forehead. Physical examination revealed a semiflucuant 1.5 cm mass with normal overlying skin. There was no pulsation, palpable thrill, or audible bruit. There were also no local inflammatory signs or neurological deficits. Patient recalled no any history of local trauma. Clinical impression was a lipoma. The patient underwent an excisional biopsy.
Microscopically, the overlying epidermis was normal. In the deep dermis, proliferating mature blood vessels were seen to dissect between the skeletal muscle fibers with focal degeneration of muscle bundles, focal fibrosis and chronic inflammation. Foci of adipose tissue were also noted intermingling with blood vessels (Figure 1 & 2). There was no endothelial atypia. A diagnosis of intramuscular angioma was made.
Figure 1
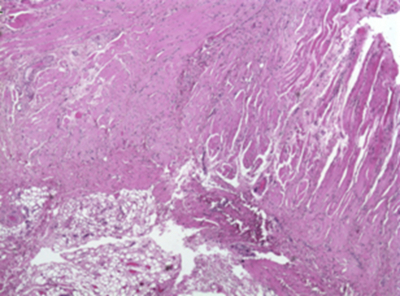
Figure 2

Comment
The origin of intramuscular angiomas remains unclear, although abnormal embryonic tissue sequestration and trauma have been postulated[3]. At present, minor trauma is considered to be a trigger factor. The resulting increase of local blood flow can initiate proliferation of the locally trapped embryonic vascular tissue to form a collection of blood vessels, leading to a hemangiomatous lesion. The trauma is usually evidenced by the muscle degeneration,focal calcification or ossification, which are common features of intramuscular angiomas.
Microscopically, the appearance of intramuscular angiomas is variable, partially due to the mixed features of vessel components. The most common type of lesion involves prominent, thick-walled, muscular veins, together with a mixture of capillary and cavernous-size vessels as well as lymphatic vessels. Thus, the term angioma, instead of hemangioma is the preferred[4]. Most of the intramuscular angiomas have a prominent adipose component, which frequently leads to a misdiagnosis of lipoma[5]. Whether the adipose tissue is an intrinsic element of the lesion, or the product of muscular degeneration and atrophy, remains uncertain.
The treatment of the intramuscular angiomas depends on the location and clinical symptoms. The patient may require a surgical excision for a tumor that is large with intractable pain for cosmetic reason. A complete excision with a clear margin is preferred, because the local recurrence rate can be as high as 18% after incomplete removal[6].
Correspondence to
Deba P Sarma, M.D. Department of Pathology Creighton University Medical Center 601 North 30th Street Omaha, NE 68131 Email: debasarma@creighton.edu